The Step 1 examination continues to assess content related to the discipline of pharmacology. However, the primary focus of this content will be on the mechanisms of actions of drugs rather than on specific pharmacotherapy, drug-drug interactions, adverse effects, or contraindications of medications.
A 27-year-old woman comes to the office for counseling prior to conception. She states that a friend recently delivered a newborn with a neural tube defect and she wants to decrease her risk for having a child with this condition. She has no history of major medical illness and takes no medications. Physical examination shows no abnormalities. It is most appropriate to recommend that this patient begin supplementation with a vitamin that is a cofactor in which of the following processes?
(A) Biosynthesis of nucleotides
(B) Protein gamma glutamate carboxylation
(C) Scavenging of free radicals
(D) Transketolation
(E) Triglyceride lipolysis
(Answer: A)
The Step 1 examination includes items pertaining to the understanding of the principles of biostatistics and epidemiology, including principles of research ethics and regulatory issues.
A study is designed to evaluate the feasibility of acupuncture in children with chronic headaches. Sixty children with chronic headaches are recruited for the study. In addition to their usual therapy, all children are treated with acupuncture three times a week for 2 months. Which of the following best describes this study design?
(A) Case-control
(B) Case series
(C) Crossover
(D) Cross-sectional
(E) Historical cohort
(F) Randomized clinical trial
(Answer: B)
A 42-year-old nulligravid woman comes to the office because of a 1-year history of increasingly irregular vaginal bleeding and menstrual cramps. Previously, menses occurred at regular 28-day intervals and lasted 3 days with minimal cramping. During the past year, menstrual periods have occurred at 21- to 28-day intervals and lasted 10 to 12 days with increasingly severe pain. Use of acetaminophen and ibuprofen has provided minimal relief. She used an oral contraceptive from the age of 17 years to 40 years, but she discontinued use after she was diagnosed with deep venous thrombosis of the right lower extremity. She has no other history of serious illness and takes no medications. Her mother and sister underwent hysterectomy at the ages of 39 and 43 years, respectively, because of abnormal uterine bleeding. The patient is 163 cm (5 ft 4 in) tall and weighs 75 kg (165 lb); BMI is 28 kg/m2. Vital signs are within normal limits. Physical examination discloses an enlarged, irregularly shaped uterus with nodularity. Which of the following is the most likely cause of the patient’s symptoms?
(A) Benign monoclonal tumors arising from smooth muscle cells
(B) Endometrium growing into the myometrium
(C) Endometrium growing outside the uterus
(D) Failure of functional ovarian cysts to regress after the release of an ovum
(E) Ovarian stromal cells dividing and multiplying rapidly
A 6-year-old boy is brought to the office by his mother because of a 1-month history of bleeding gums after brushing his teeth, increasingly severe muscle and joint pain, fatigue, and easy bruising. His mother says he has lost six baby teeth and has been irritable during this time. Use of acetaminophen has provided minimal relief of his pain. He has autism spectrum disorder. He is not toilet-trained. He has a 10-word vocabulary. Vital signs are within normal limits. On examination, he appears alert but does not speak or make eye contact. Skin is pale and coarse. Examination of the scalp shows erythematous hair follicles. Dentition is poor, and gingivae bleed easily to touch. Multiple ecchymoses and petechiae are noted over the trunk and all extremities. There is marked swelling and tenderness to palpation of the elbow, wrist, knee, and ankle joints. He moves all extremities in a limited, guarded manner. Deep tendon reflexes are absent throughout. It is most appropriate to obtain specific additional history regarding which of the following in this patient?
(A) Diet
(B) Evidence of pica
(C) Herbal supplementations
(D) Lead exposure
(E) Self-injurious behaviors
(Answer: A)
A 28-year-old man comes to the office because of a 1-year history of pain with urination that has increased in severity during the past month. He also has had episodes of blood in his urine during the past 5 years. He lived in sub-Saharan Africa until he came to the USA 6 months ago for graduate school. Temperature is 38.0°C (100.4°F), pulse is 80/min, respirations are 16/min, and blood pressure is 110/84 mm Hg. Physical examination shows suprapubic tenderness. Laboratory studies show:
| Hemoglobin | 12.3 g/dL |
| Hematocrit | 37% |
| Leukocyte count | 13,400/mm3 |
| Segmented neutrophils | 65% |
| Bands | 5% |
| Eosinophils | 5% |
| Lymphocytes | 22% |
| Monocytes | 3% |
| Serum | |
| Urea nitrogen | 75 mg/dL |
| Creatinine | 3.8 mg/dL |
| Urine | |
| Blood | 3+ |
| RBC | 200/hpf |
| WBC | 100/hpf |
| RBC casts | absent |
| WBC casts | absent |
Imaging studies show bilateral hydroureter and hydronephrosis and foci of calcification in the region of the bladder. A biopsy specimen of the bladder shows marked chronic inflammation with fibrosis and scattered granulomas. Which of the following best explains the biopsy findings?
(A) Exposure to a chemical toxin
(B) Interstitial cystitis
(C) Malacoplakia
(D) Schistosomiasis
(E) Vesicoureteral reflux
(Answer: D)
Осенью прошлого года ездил на курсы подготовки к USMLE Step 1 в Даллас. USMLE (United States Medical Licence Exam) – это многоступенчатый стандартизированный экзамен для поступления в медицинскую резидентуру, последующей сертификацией и работы врачом в США.
Практически любой кто закончил медицинскую школу за пределами Америки, может попытаться сдать этот экзамен.
Многие признают, что Step 1 является самым трудным из существующих (не только медицинских) экзаменов в мире. Складывается это из несколько причин:
Во-первых, конкуренция. Usmle сдают лучшие выпускники медицинских вузов со всего мира (особенно Индии, Китая, Ирана, Пакистана, Великобритании, Канады). Поэтому постоянно задирается планка проходного балла (passing score). Например, 8 лет назад проходной балл для Step 2 CK был 165, сейчас 203.
Во-вторых, элитарность и деньги. Врачебная специальность в США является самой оплачиваемой специальностью и самой престижной. Ежегодный средний доход терапевта 175 тысяч долларов в год, анестезиолога 360 тысяч, а ортопеда выше 400 (источник: Medscape).
Многие хотят быть врачами в США, поэтому существует такой жесткий фильтр как USMLE.
Лучший процент студентов сдающих экзамен на проходной балл, – в американских школах, официально 97% т.е. 97% студентов сдают экзамен. На самом деле сдают примерно 85%. Остальных 10-15% студентов отчисляли якобы по собственному желанию (официальные цифры 6%) .
Мне всегда было трудно понять, как человек который с 14 лет готовится поступить в колледж, платит за 4 года в колледже около 160 тысяч $, делает premed, отказывает себе во всем, сдает MCAT, поступает в медицинскую школу платя за нее как минимум 50 тысяч в год, вдруг после второго курса бросает. Оказывается, для большинства школ, студентам нужно получить допуск на экзамен USMLE, предварительно пройдя претест NBME. Тех кто его заваливал этот претест, отчисляли из ВУЗа, поэтому они не шли в статистику не сдавших экзамены. Отсюда такой высокой процент сдающих 97%.
Самый маленький процент сдающих USMLE дают школы карибского бассейна. Из них самые слабые Winsdor и Sr. Kittis по неофициальным данным 18%. Таким образом, 82% студентов отчисляются после второго года обучения.
Сам экзамен USMLE – это тест на компьютере на 8 часов. Вопросы очень сложные. Очень мало вопросов прямых, на каждый вопрос нужно думать. Примерно как IQ, но по медицине. Приведу очень легкий пример вопроса:
Белый мужчина 40 лет взял новый не использованный экспресс тест на беременность своей жены и окунул в свою мочу. Тест показал, что мужчина беременный. Какая у него профессия?
A. Дворник
Б. Водитель
В. Полицейский
Г. Инженер атомной электростанции
Д. Санта-Клаус
Как решить. Тест на беременность определяет наличие хорионического гонадотропина (ХГЧ). Если он положительный, то женщина беременна. У беременных ХГЧ выделяет плацента (синцитиотрофобласт). В нашем случае, мы имеем мужчину у которого точно в моче есть ХГЧ. Возможно у него рак яичек – хориокарцинома – трофобластическая опухоль, развивающаяся в результате злокачественной трансформации эпителия хориона при которой повышен уровень ХГЧ. Предположительный диагноз мы знаем, но вопрос о профессиях. Вспоминаем, хориокарцинома чаще встречается у трубочистов. Смотрим ответы… наиболее близкий вариант Санта Клаус (он же лазит по дымовым трубам). Правильный ответ д.
Второй вопрос. Этот же больной. Что из нижеперечисленного, вы будете наблюдать у этого пациента?
A. гипертония
Б. гипотония
В. гипертиреоидизм
Г. гипотиреоидизм
Д. гипергонадизм
Е. гипогонадизм
Решение. ХГЧ по структуре сходен с тиреостимулирующим гормоном (ТСГ). Повышенный ХГЧ может стимулировать рецепторы ТСГ. Повышенный ТСГ повышает тиреоидные гормоны, которые по обратной связи будет снижать ТСГ и релизинг гормон. Таким образом, мы можем наблюдать гипертиреоз. Ответ В.
Не важно, что пример не совсем реальный, важно, что студент на основе своих знаний пришел к правильным вариантам. Вопросы всегда разные и обычно они на пол страницы.
Как я готовился.
Я начал свою серьезную подготовку в августе 2012, сдал экзамен 3 декабря 2013.
Я пытался выучить медицину, как учат в России, но у меня не получилось. Я сделал претест и получил 18% правильных ответов (нужно 75%). Если посадить первоклассника, то он ответит на 10-15%. Просто будет кликать на любые ответы.
В итоге я решил понять медицину, как работает наш организм, от молекулярной биологии до физиологии. Последний претест (NBME #7) сдал с результатом в 78% правильных ответов (score 212).
Что я сделал?
1. Посмотрел видео лекции:
-Каплановские 380 часов
– Доктор Саттар 60 часов
2. Прочитал книги:
– Каплановские 7 книг (Анатомия, Биохимия, Фармакология, Физиология, Патология, Бихевиористика, Иммунология, Микробиология) – 3 200 страниц
– Беккеровские 7 книг (Анатомия, Биохимия, Фармакология, Физиология, Патология, Бихевиористика, Иммунология, Микробиология, ) – 3 600 страниц
– Патология Гольян 650 страниц
– Издание High Yeld (Анатомия, Биохимия, Фармакология, Физиология, Патология, Бихевиористика, Иммунология, Микробиология, Генетика, Эмбриология) – 2 400 страниц
– Клиническая микробиология Made Ridiculously simple – 600 страниц
– Патология издание BRS – 580 страниц х 2 раза = 1060 страниц
– Физиология издание BRS – 480 страниц
– Usmle Step 1 Q&A –600 страниц
– USMLE Step 1 Cases – 600 страниц
– Патология (“маленький” Робинс) осилил только 200 страниц
– First Aid – 564 страницы х 3 раза = 1 692 страницы

3. Решил тесты: (1 вопрос и объяснение = 1 страница)
– Каплановский Q банк – 2 300 вопросов
– UWorld – 2 200
– Usmle QRAX – осилил только 2 тыс из трех
– NBME (6 штук по 200 каждый) – 1200
4. Прошел курсы:
– Каплановские 14 недель
– Беккеровские 7 недель
Итого за 18 месяцев:
Просмотрел – 440 часов лекций
Прочитал – 14 482 страницы
Решил – 7 700 вопросов
Живых лекций – 668 часов
После того, как я исписал все тетради в доме, я стал делать заметки прямо в книгах. Каждая страница у меня выглядит так

Я знаю, что некоторые умудряются сдать прочитав две книги за два месяца, но видимо это не я.
Доктор Гольян (Edward Goljan)
На Далласовских курсах познакомился с богом патологии и 10 кратным лучшим профессором США (в категории basic science), 9 кратным обладателем Golden Apple – доктором Гольян. Мало того, что он написал бестселлер Патология переживший уже четыре издания, но и он являлся чемпионом штата Оклахома по армрестлингу среди профессионалов.
На доктора Гольяна съехались медицинские студенты практически со всей страны. За ним постоянно бегали, фотографировались, брали автографы. Мне даже казалось, что это не профессор, а какая-то кино-звезда.
Отрывок письма, которое я получил по поводу лекции Гольяна
Goljan will start at 7:45am the first day and last day (Sunday 9/29 and Friday 10/4)
All other days class is from 8:00 – 6:00 pm. Q/A session is from 6:00 – 7:00 pm.
The classroom doors will be open at 6:45am
-Please refrain from bringing: backpacks, purses, etc. (Use Ziploc bags for those things like highlighters, snacks, etc.)
–IDs must be visible at all times
–No coming in and out of the classroom while Dr. Goljan is lecturing
-No saving seats or talking during class
We’d like to remind all of you that NOlaptops, PHONES or recording devices are allowed in the classroom
Как видно из инструкции, на лекцию запрещено приносить любые электронные приборы, сотовый телефон, сумки, рюкзаки, вообщем можно только книгу, тетрадь, ручку и бутерброд в прозрачном пакете. Нельзя выходить и заходить в лекционный зал во время лекции. Нельзя разговаривать.
За час до лекции в конференц зал нельзя было пробиться, драка была за первые парты. Вызывали охрану. Во время лекции стояла полная тишина, иногда прерывающаяся на аплодисменты или восторженные вопли WOW. После объяснения ЭКГ и различных аритмий моя соседка по парте зарыдала со словами: “he is f***ing awesome”.
Меня поразил Гольян не только своим феноменальным умом и профессионализмом, но и своей отличной физической формой (мужику 70 лет). В перерывах между лекциями он качал пресс, отжимался на одной руке. Не выдержав искушения после очередной лекции, я прождав к нему очередь больше 2 часов сфотографировался.

На фото не видно, что он очень здоровый, вот видео (напомню, профессору 70 лет)
В США я понял наконец таки пословицу – ЗНАНИЕ – СИЛА!
FREE USMLE® PRACTICE
GET STARTED ON YOUR STUDY PLAN—FOR FREE
USMLE Question of the Day
Get a little practice every day with our daily exam-style questions.
Answer Today’s Question
Qbank Free Trial
Not all Qbanks are created equal. Only Kaplan can provide you with a true exam-like interface. Don’t just take our word for it— try our Qbank right now for free.
Learn More
Qbank Integrated Plan Free Trial
When you combine Kaplan’s renowned Qbank with 70 hours of online instruction, 2 full-length simulated exams, and 26 mastery assessments, you get all-inclusive integrated practice.
Learn more
On Demand Prep Free Trial
Within the trial you’ll get access to our best videos and sample our new warm-up and post-test questions.
Learn More
Free Step 1 Diagnostic Exams
Kaplan’s free USMLE Step 1 Diagnostic test is 3-hours in length and provides you with detailed feedback showing how you did overall and on individual disciplines.
Learn More
USMLE Advising Sessions
Schedule a free 20-minute session with one of our advisors. They know every exam and every part of the medical residency application timeline. Why not try it?
Schedule a Call
Free Practice Questions
READY TO GET STARTED?
Take a USMLE class led by a teacher—online or in person. Or pace your own prep. No matter what stage of test prep you’re in, we can help raise your score.
Are you preparing for the USMLE® Step 1 or 2 CK? Try free practice questions below or access more questions for all major Step 1 and Step 2 CK topics in Lecturio’s all-in-one USMLE Qbank.
Learning From Clinical Cases
As a medical student, you’ll spend a lot of time learning about medicine, practicing with cadavers, and eventually training a hospital with real patients. But before you put on your white coat and start taking vitals, you’ll likely go through thousands of USMLE® practice questions.
On the USMLE® Step 1 and Step 2 CK exams, you’ll encounter between 280 and 318 patient-centered clinical vignettes paired with multiple choice answers. These clinical cases will require multi-step thinking and some will also require you to interpret graphic or pictorial materials. These are single best answer questions, so while multiple answers may be partially correct, each question only has one best answer.
Free USMLE® Step 1 Questions
![]()
Free USMLE® Step 2 Questions
Beat the Boards: 30 USMLE Question Walkthroughs

![]()
Familiarize yourself with how to best approach USMLE Qbank questions
![]()
Learn important tricks for tackling the stems of USMLE questions
![]()
Assess your current state of knowledge of various USMLE Step 1 question topics
You can then study using Lecturio’s subject-based study schedules or create custom Qbank tests in either “tutor” or “test” mode. Doing a Lecturio Qbank block in “tutor mode” provides detailed answer explanations and connects you to related videos and resources, including First Aid® page references so that you can study as you go. Doing a Lecturio Qbank block in “test mode” simulates your exam day experience, from the time pressure to the interface of the test itself.
Don’t Cram—Start Studying Smarter with Lecturio’s all-in-one Qbank!
1
Take & review
your Qbank test
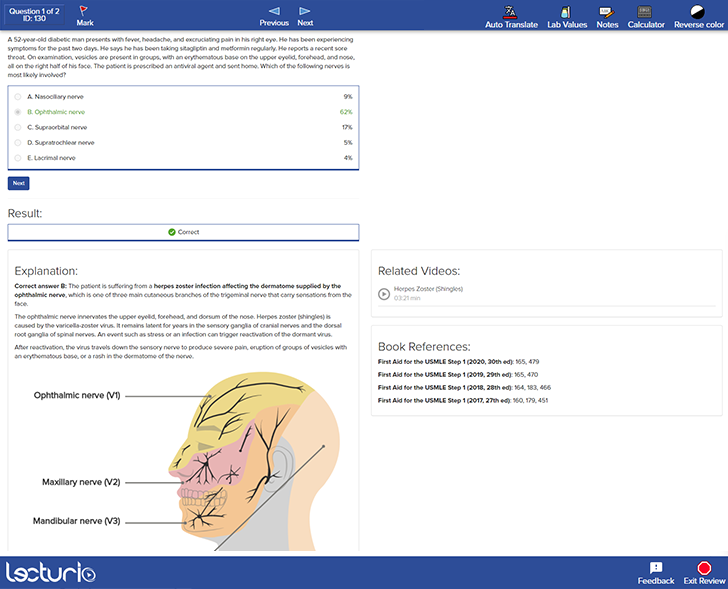
2
Check the up-to-date First Aid® references & take notes

3
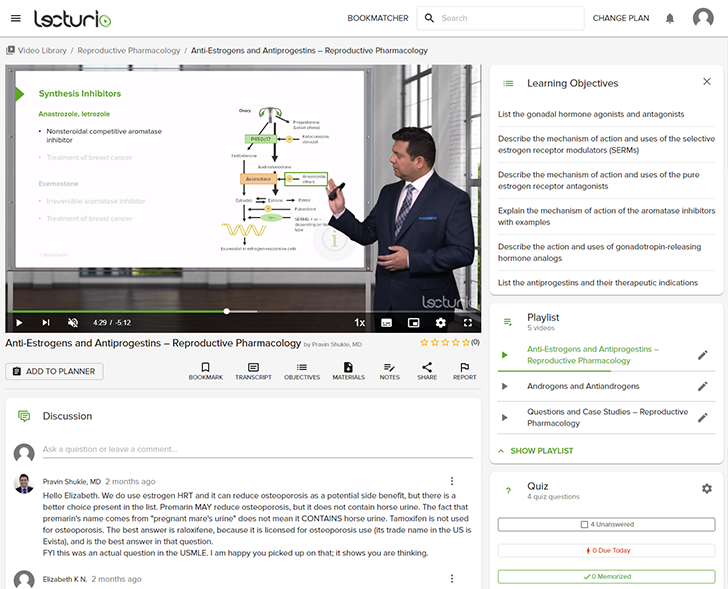
Learn with integrated high-yield video lectures
Keep up the Practice with the USMLE® Question of the Day
Get a new daily USMLE® question sent to you every morning and benefit from detailed answer explanations.

![]()
Learn anywhere and anytime—even when you‘re offline
![]()
The Bookmatcher turns your textbook into explanatory video lectures
![]()
Available for Android and iOS
![]()
![]()
Preview 10 Free USMLE® Step 1 Questions
A 25-year-old man is admitted to the hospital after a severe motor vehicle accident as an unrestrained front-seat passenger. Appropriate life-saving measures are given, and the patient is now hemodynamically stable. Physical examination shows a Glasgow Coma Score of 12. There are no motor or ocular movements with painful stimuli. The patient has bilaterally intact pupillary light reflexes. The patient is placed in a 30° semi-recumbent position for further examination. What is the most likely finding on the examination of this patient’s right ear?
A. Cold water causing ipsilateral saccadic movement
B. Warm water causing an ipsilateral slow pursuit
C. Warm water causing ipsilateral saccadic movement
D. Warm water mimicking the head-turning left
E. Cold water causing contralateral slow pursuit
A 50-year-old man presents to the office with complaints of fever and chills for 4 weeks. He adds that he is fatigued all the time and has a generalized weakness. He has drenching night sweats and has had 2 episodes of non-bilious vomiting over the past few days. He traveled to the Netherlands for 4 days a month ago. His symptoms started a few days after he returned home. Laboratory testing revealed the following:
| Hemoglobin | 11.2 g/dL |
| Hematocrit | 29% |
| Leukocyte count | 2,950/mm3 |
| Neutrophils | 59% |
| Bands | 3% |
| Eosinophils | 1% |
| Basophils | 0% |
| Lymphocytes | 31% |
| Monocytes | 4% |
| Platelet count | 60,000/mm3 |
| Unconjugated bilirubin | 12 mg/dL |
| Alanine aminotransferase | 200 IU/L |
| Aspartate aminotransferase | 355 IU/L |
The peripheral blood smear showed basophilic ring- and pear-shaped structures inside many red cells and extracellular basophilic rings on Wright-Giemsa staining. Further evaluation revealed parasitemia and a few schistocytes, poikilocytes, and merozoites in tetrad formation. The findings are most consistent with which diagnosis?
A. Malaria
B. Babesiosis
C. Anaplasmosis
D. Tuberculosis
E. Lyme disease
A 22-year-old professional softball player is undergoing an annual check-up. Her medical history is significant for hallux valgus and scoliosis. She additionally notes that she frequently has bumps and bruises from playing softball, but she has no injuries today. Her family history is significant for heart disease. The patient’s blood pressure is 110/70 mm Hg, heart rate is 78/min, and respiratory rate is 15/min. A physical examination is unremarkable except for an indurated palpable mass on her left breast. A biopsy of the mass is performed. Which biopsy findings are most likely to be present in this patient?
A. Chronic inflammation with plasma cells
B. Necrotic fat with calcifications and giant cells
C. Leaf-like projections
D. Duct-like structures
E. Abundant extracellular mucin
A 55-year-old woman presents to the office because she has been feeling weak. For the past 2 years, she has been urinating a considerable volume every time she goes to the bathroom. She has no past medical history. Her heart rate is 86/min, respiratory rate is 15/min, temperature is 37.4°C (99.3°F), and blood pressure is 111/79 mm Hg. Laboratory studies are significant for the following:
| Calcium | 13.8 mg/dL |
| PTH | 230 pg/mL |
Her complete metabolic panel is otherwise within normal limits. Imaging studies show subperiosteal resorption and osteoporosis. Scintigraphy reveals the most common pathologic condition associated with the patient’s diagnosis. Which of the following is the most likely diagnosis in this patient?
A. Adenoma
B. Carcinoma
C. Decreased calcitriol concentration
D. Glandular hyperplasia
E. Phosphate retention
A 48-year-old man is brought to the emergency department by his neighbor, who found him lying unconscious at the door of his house. The patient lives alone and no further history is available. On physical examination, his temperature is 37.2ºC (98.9ºF), pulse rate is 114/min, blood pressure is 116/78 mm Hg, and respiratory rate is 22/min. His Glasgow Coma Scale score is 7 and the patient is intubated. A stat serum osmolality is reported at 260 mmol/kg. Based on the provided information, which of the following conditions is most likely present in this patient?
A. Acute ethanol intoxication
B. Central diabetes insipidus
C. Diabetic ketoacidosis
D. Nonketotic hyperosmolar hyperglycemic coma
E. Syndrome of inappropriate antidiuretic hormone
A 40-year-old woman with a recent history of carcinoma of the breast status-post mastectomy and neoadjuvant chemotherapy 1 week ago presents for follow-up. She reports adequate pain control with the analgesic drug she was prescribed. Her past medical history is significant for hepatitis C and major depressive disorder. The patient denies any history of smoking or alcohol use but says she is currently using intravenous heroin and has been doing so for the past 10 years. However, she reports that she has been using much less heroin since she started taking the pain medication, which is confirmed by the toxicology screen. Which of the following is the primary mechanism of action of the analgesic drug she was most likely prescribed?
A. Partial agonist at opioid receptors
B. Pure antagonist at opioid receptors
C. Inhibits prostaglandin synthesis
D. Pure agonist at the µ-opioid receptor
E. Central action via blockade of serotonin reuptake
A 60-year-old man seeks evaluation at a medical office due to leg pain while walking. He says the pain starts in his buttocks and extends to the thighs and down to the calves. Previously, the pain resolved with rest, but the pain now persists in his feet, even during rest. The past medical history is significant for diabetes mellitus, hypertension, and cigarette smoking. The vital signs are within normal limits. The physical examination shows an atrophied leg with bilateral loss of hair. Which of the following is the most likely cause of this patient’s condition?
A. Decreased permeability of endothelium
B. Narrowing and calcification of vessels
C. Peripheral emboli formation
D. Thrombus formation
E. Weakening of vessel wall
A 33-year-old woman presents with lethargy and neck pain. She says that, for the past 6 months, she has been feeling tired all the time and has noticed a lot of muscle tension around the base of her neck. She also says she finds herself constantly worrying about everything, such as if her registered mail would reach family and friends in time for the holidays or if the children had their nightly baths while she was away for the weekend. She says that this worrying has prevented her from sleeping at night and has made her more irritable and edgy with her family and friends. Which of the following is the best course of treatment for this patient?
A. Buspirone
B. Diazepam
C. Family therapy
D. Support groups
E. A vacation
A healthy 37-year-old gravida-3-para-1 (G-3-P-1) who underwent in vitro fertilization delivers a boy vaginally. On examination, he is found to have a ventral urethral meatus inferior to the glans. Which statement is correct?
A. Younger age of the mother is a major risk factor for this condition
B. It results from failure of the genital swellings to fuse
C. Hypospadias repair before the age of 3 years is associated with an increased incidence of urethrocutaneous fistula
D. Such anatomy is formed before the 12th week of intrauterine development
E. It results from failure of the urethral folds to fuse
Parkinson’s disease is a progressive neurodegenerative disease. It is characterized by a loss of dopaminergic neurons in the substantia nigra pars compacta and the formation of cellular inclusions called Lewy bodies. These are composed of α-synuclein that has been bound to ubiquitin. In healthy individuals, α-synuclein bound to ubiquitin would be degraded by which of the following?
A. Vesicle
B. Peroxisome
C. Proteasome
D. Ribosome
E. Lysosome
Do you want to practice more USMLE Step 1 questions?
Create a free Lecturio account and you’ll access the Lecturio question bank, with more than 2,200 USMLE Step 1 practice questions.
Preview 10 Free USMLE® Step 2 Questions
A 65-year-old man is brought to the emergency department after losing consciousness. He is accompanied by his wife. He is started on intravenous fluids. His vital signs are blood pressure 85/50 mm Hg, pulse 50/min, and respiratory rate 10/min. He has been admitted in the past for a heart condition. His wife is unable to recall the name of the condition, but she does know that the doctor recommended some medications at that time in case his condition worsened. She has brought with her the test reports from previous medical visits over the last few months. She says that she has noticed that he often has difficulty breathing and requires three pillows to sleep at night to avoid being short of breath. He can only walk for a few minutes before he has to stop and rest. His wife also reports that he has had occasional severe coughing spells with pinkish sputum production. She also mentions that he has been drinking alcohol for the past 30 years. Which of the following medications will improve the prognosis of this patient?
A. Furosemide
B. Enalapril
C. Digoxin
D. Amiodarone
E. Amlodipine
A 2-year-old boy is presented to the pediatrician with poor weight gain and fatigue. His mother states that the patient barely engages in any physical activity because he easily becomes short of breath. His prenatal and birth histories are insignificant. The patient’s past medical history includes a few upper respiratory tract infection episodes that were treated successfully. He is in the 10th percentile for weight and 40th percentile for height. His heart rate is 122/min, blood pressure is 102/56 mmHg, and respiratory rate is 32/min. Cardiac auscultation reveals clear lungs and a grade 2/6 holosystolic murmur that is loudest at the left lower sternal border. The remainder of the physical examination is negative for clubbing, cyanosis, and peripheral edema. Which of the following is the most likely diagnosis in this patient?
A. Patent ductus arteriosus (PDA)
B. Atrial septal defect (ASD)
C. Ventricular septal defect (VSD)
D. Coarctation of the aorta
E. Tetralogy of Fallot (TOF)
A 36-year-old primigravida presents to her obstetrician for antenatal care. She is at 26 weeks of gestation and does not have any current complaints except for occasional leg cramps. She does not smoke or drink alcohol. Family history is irrelevant. Her temperature is 36.9°C (98.42°F), the blood pressure is 100/60 mm Hg, and the pulse is 95/minute. Her body mass index is 21 kg/m² (46 pounds/m²). Physical examination reveals a palpable uterus above the umbilicus with no other abnormalities. Which of the following screening tests is suitable for this patient?
A. HbA1c for gestational diabetes mellitus
B. Oral glucose tolerance test for gestational diabetes mellitus
C. Fasting and random glucose testing for gestational diabetes mellitus
D. Wet mount microscopy of vaginal secretions for bacterial vaginosis
E. Complete blood count for iron deficiency anemia
A 52-year-old man presents to the emergency department because of bilateral leg swelling and puffiness of both eyes in the morning. His symptoms started about 2 weeks ago. He denies smoking or alcohol use and his family history is noncontributory. The vital signs include: temperature 36.8°C (98.2°F), blood pressure 162/87 mm Hg, and pulse 85/min. On physical examination, he is jaundiced and there is hepatosplenomegaly and 2+ lower extremity edema up to the mid-thigh. Laboratory studies show:
| Anti-HCV | Reactive |
| Serum albumin | 3 g/dL |
| Urine dipstick | 3+ protein |
| Urinalysis | 10–15 red blood cells/high-power field (RBCs/HPF) and red cell casts |
Which of the following is a feature of this patient’s condition?
A. Subendothelial immune complex deposits
B. Phospholipase A2 receptor antibodies
C. Normal complement level
D. Renal vasoconstriction and altered autoregulation
E. Few immune complex deposits
A 43-year-old woman was admitted to the hospital after a fall. When the emergency services arrived, she was unresponsive, did not open her eyes, but responded to painful stimuli. The witnesses say that she had convulsions lasting about 30 seconds when she lost consciousness after a traumatic event. On her way to the hospital, she regained consciousness. On admission, she complained of intense headaches and nausea. She opened her eyes spontaneously, was responsive but confused, and was able to follow motor commands. Her blood pressure is 150/90 mm Hg, heart rate is 62/min, respiratory rate is 13/min, and temperature is 37.3℃ (99.1℉). There are no signs of a skull fracture. The pupils are round, equal, and poorly reactive to light. She is unable to fully abduct both eyes. Ophthalmoscopy does not show papillary edema or retinal hemorrhages. She has nuchal rigidity and a positive Kernig sign. An urgent head CT does not show any abnormalities. Which of the following is the next best step for this patient?
A. Brain MRI
B. Lumbar puncture
C. Angiography
D. EEG
E. Sonography
A 15-year-old African American boy presents to the pediatrician with yellow discoloration of his sclerae for the last 3 days. His mother reports that he developed prolonged jaundice during the neonatal period. Vital signs are within normal limits. Physical exam reveals scleral icterus, mild splenomegaly, and pallor. Laboratory studies show the following:
| Hemoglobin | 9.9 g/dL |
| Total leukocyte count | 7,500/mm3 |
| Platelet count | 320,000/mm3 |
| Reticulocyte count | 5% |
| Mean corpuscular hemoglobin | 27.7 pg/cell |
| Mean corpuscular hemoglobin concentration | 32% g/dL |
| Mean corpuscular volume | 84 μm3 |
| Serum total bilirubin | 4.2 mg/dL |
| Serum direct bilirubin | 0.3 mg/dL |
| Coombs test | Negative |
Peripheral smear demonstrates polychromasia, blister cells, and Heinz bodies. Abdominal ultrasonography reveals the presence of gallstones. Which of the following tests is most likely to be abnormal for this patient?
A. Glycerol lysis test
B. Methemoglobin reduction test
C. Serum thyroxine, triiodothyronine, and thyroid-stimulating hormone
D. Serum lipoprotein-X level
E. Hepatoiminodiacetic acid scanning
A 24-year-old woman with a past medical history significant only for endometriosis presents to the outpatient clinic with a 2-cm left breast mass that she first identified 6 months earlier. On review of systems, the patient states that the mass is not painful and, by her estimation, has not significantly increased in size since she first noticed it. On physical examination, there is a palpable, round, rubbery, mobile mass approximately 2 cm in diameter. Given the lesion’s characteristics and the patient’s demographics, what is the most likely diagnosis?
A. Fibrocystic change
B. Fibroadenoma
C. Cystosarcoma phyllodes
D. Ductal carcinoma in situ
E. Invasive breast carcinoma
A 3-day-old boy is brought to the pediatrician for nonpigmented vomiting for the last day. A detailed developmental history reveals that his parents have a nonconsanguineous marriage. He was born by cesarean section at 36 weeks of gestation. His birth weight was 2.6 kg (5.7 lb), and he has been breastfed exclusively. His temperature is 37.0ºC (98.6°F), pulse is 120/min, and respiratory rate is 35/min. On physical examination, a distended abdomen and signs of dehydration are present. On abdominal imaging, a ‘double bubble’ sign and upper intestinal obstruction is present. Abdominal computed tomography shows narrowing of the second part of the duodenum. Barium enema shows normal rotation of the colon. Which of the following is most likely cause of intestinal obstruction in this patient?
A. Meckel diverticulum
B. Annular pancreas
C. Leukocyte adhesion deficiency
D. Crigler-Najjar type 1
E. Intussusception
A 22-year-old woman from a rural area who recently discovered she was pregnant is referred for a cardiology consultation due to cyanosis, dyspnea, and a cardiac murmur revealed at the initial prenatal visit. She is gravida 1, para 0 with an estimated gestational age of 19 weeks. She says that the murmur was found in her childhood, and the doctor at that time placed her under observation only. However, she has been lost to follow-up and has not had proper follow up in years. Currently, she complains of dizziness and occasional dyspnea on exertion which has gradually increased during her pregnancy. Prior to her pregnancy, she did not have any symptoms. The vital signs are as follows: blood pressure 125/60 mm Hg, heart rate 81/min, respiratory rate 13/min, and temperature 36.7°C (98.0°F). Her examination is significant for acrocyanosis and a fixed splitting of S2 and grade 3/6 midsystolic murmur best heard over the left upper sternal border. Which of the following physiological pregnancy changes is causing the change in this patient’s condition?
A. Increase in pulmonary vascular resistance
B. Increase in heart rate
C. Decrease in systemic vascular resistance
D. Increase in cardiac output
E. Increase in blood volume
A 24-year-old woman, G1P0, presents to her OB/GYN for her annual examination with complaints of painful cramps, abdominal pressure, and bloating with her cycle. She reports that she has not menstruated since her missed abortion requiring dilatation and curettage (D&C) seven months ago. She is sexually active with her husband and is not using any form of contraception. Her BMI is 29. At the clinic, her temperature is 98.9°F, pulse is 80/min, and blood pressure is 120/70 mm Hg. The physical examination is unremarkable. Thyroid-stimulating hormone, follicle-stimulating hormone, and prolactin concentrations are all within normal limits. The patient tests negative for qualitative serum beta‐hCG. A progestin challenge test reveals no withdrawal bleeding. What is the most likely diagnosis?
A. Ectopic pregnancy
B. Pelvic inflammatory disease
C. Endometriosis
D. Asherman syndrome
E. Hypothalamic hypoestrogenism
Do you want to practice more USMLE Step 2 questions?
Create a free Lecturio account and you’ll access the Lecturio question bank, with more than 1,200 USMLE Step 2 CK practice questions.
Free USMLE® Step 1 Questions by Subjects
Free USMLE® Step 2 CK Questions by Subjects

FREE USMLE Step 1 Practice Questions
Are you considering taking the United States Medical Licensing Examination (USMLE) Step 1? If so, you probably know that it’s important to get as much practice as possible before the big day. One way to do this is by working through free USMLE Step 1 practice questions.
But where can you find high-quality practice questions that will help you prepare for the exam? Here are a few options to consider:
-
The USMLE website: The official USMLE website offers a number of free practice questions that cover a variety of topics tested on the Step 1 exam. These questions are written by the same team that creates the actual exam, so you can be confident that they are representative of the types of questions you will see on test day.
-
Online study guides: There are a number of online study guides that offer free USMLE Step 1 practice questions as part of their comprehensive review materials. These questions are often accompanied by detailed explanations and references, which can help you learn more about the concepts being tested.
-
Flashcard apps: There are several flashcard apps that offer free USMLE Step 1 practice questions as part of their study materials. These apps can be a convenient way to review on the go and track your progress over time.
No matter which source you choose, it’s important to work through as many practice questions as possible in order to get a feel for the types of questions you will encounter on the exam. By doing so, you can improve your test-taking skills and increase your confidence on exam day. Good luck!
FREE USMLE Step 1 Practice Exams
Here are 50 free USMLE Step practice test from the Smash USMLE Step 1 question bank.
A 61-year-old male is admitted to the hospital with worsening shortness of breath and fatigue. Physical examination reveals dullness to percussion and decreased breath sounds in the right lung. A chest x-ray is obtained which reveals a large right-sided pleural effusion. Thoracentesis yields 250 mL of fluid with a pleural fluid protein/serum protein ratio of 0.7 and a lactate dehydrogenase level of 240 U/L. The most likely diagnosis is
protein losing enteropathy
Correct!
Wrong!
A 27-year-old male comes to the physician with skin lesions as shown in the exhibit. Physical examination reveals soft tissue crepitus and the smell of decomposing tissue. The most likely cause of these findings can also cause infection through
respiratory droplet inhalation
skin to skin transmission
Correct!
Wrong!
A 65-year-oldfemalewith end stage renal failurecomes to her physician with a rash and is diagnosed with Lyme disease. Review of her medical records reveals severe allergic reactions to penicillin and macrolides. The most appropriate treatment for this patient’s current disease is
Correct!
Wrong!
A 42-year-old female comes to the emergency department with shortness of breath and palpitations. An ECG is obtained which reveals sustained ventricular arrhythmias which are found to be unresponsive to several medications. The attending physician finally prescribes bretylium. Bretylium works by
acting as amagnesium analog
blocking beta-1 receptors
blocking calcium channels
blocking potassium channels
Correct!
Wrong!
An 18-month-old male is brought to the physician due tomental retardation andabdominal distention. Physical examination reveals enlargement of the liver and spleen. Fundoscopy reveals a cherry red spot on the macula. The most likely other finding in this patient is increased levels of
Correct!
Wrong!
A 5-month-oldmale is brought to the physician by his parents due to twitching of his facial muscles. Review of his medical records reveals that he has previously been treatedfor several episodes of Candidainfections. Physical examination reveals low set ears, hypertelorismand a shortened philtrum. The most likely additional finding in this patient is
absence of type IV hypersensitivity
decreased alpha fetoprotein
prominent telangiectasias around the eyes
Correct!
Wrong!
A 45-year-old female comes to the physician with joint pain, swelling and morning stiffness which improves with use. She also reports weight loss of 3 kg (6.6 lbs). Laboratory tests reveals the presence of serum rheumatoid factor. Before prescribing etanercept, the physician should obtain a
purified protein derivative test
Correct!
Wrong!
A 35-year-old male comes to the physician due to fatigue. He recently returned from a trip to Japan. Laboratoryresults are as follows:
Hemoglobin 9 g/dL
Mean corpuscular volume 108 fl
MCHC 33 g/dL
Mean corpuscular hemoglobin 35 pg
A peripheral blood smear is obtained which reveals enlarged red blood cells and hypersegmented neutrophils. The most appropriate pharmacologic treatment for this patient is with
Correct!
Wrong!
A 40-year-old malecomes to the emergency department due to a two-week history of a productive cough that is occasionally associated with blood. He has had similar episodes in the past. Vitals reveal a blood pressure of 140/80 mm Hg, a heart rate of 75/min, atemperature of 37.6°C (99 6°F) and a respiratory rate of 16/min.Oxygen saturation is 90% on room air. Laboratory results are as follows:
Complete blood count
Hemoglobin 11.8 g/dL
Hematocrit 35.4%
Mean Corpuscular Volume 85 µm³
Leukocytes10,000/mm³
Differential:
Neutrophils 60%
Bands 3%
Lymphocytes 25%
Monocytes 7%
Eosinophils 3%,
Liver function studies
Alanine aminotransferase 15 U/L
Aspartate aminotransferase 90 U/L
Serum chemistry
Creatinine 1.5 mg/dL
Blood urea nitrogen 23 mg/dL
Urinalysis2+ blood, red blood cell casts
The most likely other finding in this patient’s serum is
anti-basement membrane antibodies
anti-double stranded DNAantibodies
anti-mitochondrial antibodies
anti-myeloperoxidase antibodies
anti-proteinase 3 antibodies
Correct!
Wrong!
A group of research scientists are studying immunohistochemical stains used for detecting the different types of cell. The stain which is used to detect epithelial cells is
Correct!
Wrong!
A9-month-oldmale is evaluated for lactic acidosis and increased levels of serum alanine. He is diagnosed with pyruvate dehydrogenase complex deficiency and placed on a special diet by the physician.This special diet most likely consists of
Correct!
Wrong!
A 34-year-old female comes to the physician with nausea and abdominal pain. She indicates that the pain is epigastric and it improves with food intake. She also reports recent weight gain. A urease breath test is obtained which is positive.The most likely cause of these findings has all the following characteristics except
Correct!
Wrong!
A study is conducted by researchers to determine the mechanism of action of a newly isolated hormone. Previous studies have shown that the hormone increases gene expression of growth-inducing proteins. The hormone also appears to be lipophilic and is produced upon demand rather than being stored in cell vesicles. This hormone most likely activates
phospholipase C mediated receptors
tyrosine kinase receptors
unidentified G protein coupled receptors
Correct!
Wrong!
A 65-year-old malewho had a cholecystectomy at a local hospital experiences nausea and vomiting two days later. He is prescribed metoclopramide by the resident physician. Metoclopramide is contraindicated in patients with
Correct!
Wrong!
A 34-year-old female comes to the physician with nausea and abdominal pain. She indicates that the pain is epigastric, and it improves with food intake. She also reports recent weight gain. A urease breath test is obtained which is positive.This patient is most likely at an increased risk for developing
Correct!
Wrong!
A 30-year-oldCaucasian male with HIV/AIDS develops right-sided weakness involving hisright leg. A MRI of his brain revealsmultiple ring enhancing lesions within the white matter in his left frontal lobe. The most likely source of this infection in the United States is
Correct!
Wrong!
A 35-year-old male comes to the physician due towatery diarrhea of two weeks’ duration. He also has a low-grade fever, fatigue and weight loss of 5kg (11 lbs) over thepast month. Laboratory findings include a CD4+ T cell count 70 cells/mm³. The most likely diagnosis is
Correct!
Wrong!
A 30-year-oldfemaleis brought to the emergency department after being involved in a motor vehicle accident. She was not wearing a seatbelt and was ejected from her car seat upon collision with a tree. Physical examination reveals several lacerations on her face and chest as well as an inability to open her mouth against resistance.The muscle which was most likely injured is the
Correct!
Wrong!
A 19-year-old female is brought to the emergency department after she collapsed while jogging. She has a history of anorexia nervosa. When she regains consciousness, she says as she was jogging she became lightheaded, broke out into a sweat, and had palpitations. Her fingerstick glucose is 40 mg/dL. Her palpitations and diaphoresis were most likely caused by
Correct!
Wrong!
A 15-year-old femaleis brought to the physician by her mother because she is concerned that she has not started menstruating. Physical examination reveals the patient's vagina is very shallow without a palpable uterus. There are also palpable masses in the labia majora. Karyotype analysis reveals a 46, XY genotype. Which of the following was most likely present during the early fetal life of this patient?
Decreased androgen levels
Mullerian inhibiting factor
Correct!
Wrong!
A 50-year-old male with AIDS develops a fever, headache and stiff neck. A sample of his cerebrospinal fluid reveals the presence of lymphocytes, glucose levels of 35 mg/dL and protein levels of 75 mg/dL. The test which would most likely confirm this patient’s diagnosis is the
latex particle agglutination test
polymerase chain reaction test
Correct!
Wrong!
A 35-year-old female comes to the physician due toheadaches of two months’ duration. She has no history of pre-existing medical illnesses. Vital signs are within normal limits. A head CT revealsa mass above the left petrous bone and biopsy reveals a malignant schwannoma on the left trigeminal nerve. The patient undergoes surgery for resection of the mass. If there is damage to the involved nerve during the surgery, there will be
decreased accommodation in the left eye
decreased corneal reflex in the left eye
decreased taste from the anterior two thirds of the tongue
inability to adduct the left eye
Correct!
Wrong!
A 45-year-old female comes to the physician because of headaches and palpitations. Vitals reveal a blood pressure of 190/140 mm Hg and a heart rate of 105/min. A CT scan of the abdomen is obtained which reveals an adrenal mass. The hormones secreted by the adrenal mass are derived from
Correct!
Wrong!
A 24-year-old female comes to the physician due tourinary frequency and burning with urination. She is diagnosed with a urinary tract infection and prescribed ciprofloxacin. The exposure of a fetus to ciprofloxacin can result in
Correct!
Wrong!
A 3-year-oldmale is brought to the physician due to an enlarging abdominal mass. Physical examination reveals a mass in the left abdomen that does not cross the midline. Ophthalmic examination is unremarkable. Microscopic examination of a biopsy specimen from the abdomen reveals dense immature islands of epithelial cells, ribbons of spindle fibroblastic stromal cells and poorly formed tubular structures. The most likely diagnosis?
embryonal rhabdomyosarcoma
Correct!
Wrong!
A 12-year-old female is brought to the physician by her mother due to a severe sore throat. She has significant pain with swallowing and generally feels tired. Her motheralso reports that the patient has had a high fever for the past four days. Physical examination revealsan erythematous patch on the upper posterior pharynx and tenderness of the cervical lymph nodes. Vitals reveals a temperature of 39.5°C (103.1°F). The nerve responsible for this patient's throat pain is also involved in
head rotation to opposite side
movement of intrinsic tongue muscles
sensation of the lower jaw
sensory input from carotid sinus baroreceptors
taste in the anterior two thirds of the tongue
Correct!
Wrong!
A 50-year-old male comes to the physician complaining of neck masses that have been increasing in size for the past six months. He denies having any fevers or night sweats. Physical examination revealsbilateral, nontender cervical lymphadenopathy and hepatosplenomegaly. Biopsy of a cervical node reveals architectural distortion of the lymph node with proliferation of enlarged germinal follicles. Flow cytometry reveals a predominant cell population of CD10+, CD19+ and CD20+ cells. The most likely cause of these findings is
Correct!
Wrong!
A 1-week-old maleis brought to the emergency department by his mother due to persistent crying and bloody diarrhea. She says he was delivered at 33 weeks’ gestation and has been bottle-fed since then. Physical examination reveals a rigid abdomen. The neonate undergoes emergency surgery to resect a portion of his small intestine during which bowel perforation is confirmed. Microscopic examination of the excised bowel will most likely reveal
thickened collagenous bands
Correct!
Wrong!
A 6-year-old maleis broughtto the physician due to asore throat, fever and malaise. Physical examination reveals an erythematous tongue and a sandpaper-like body rash.This most likely sequelae of this infection includes all of these except
Correct!
Wrong!
A 17-year-oldfemale is brought to the emergency department by her parents dueto right foot pain. She denies recent trauma and has no history of major illnesses. She is physically active and walks for at least one hour daily. She says that she is doing well in high school and gets along well with her parents except that they keep tellingher to eat more especially since her boyfriend broke up with her a year ago.Vitals reveal a weight 47.6 kg (105 lbs) and BMI of16 kg/m². The most likely diagnosis is
injured medial ankle tendon
Correct!
Wrong!
A 40-year-old male comes to his physician due to progressive muscle weakness and paralysis. Over the next few years, his condition progresses to complete paralysis of all voluntary muscles and he eventually dies of respiratory failure. Microscopic examination of tissue obtained at autopsy shows that both upper and lower motor neurons are degenerated. Of the listed options, the location which would likely reveal the most marked neuronal loss is the
Correct!
Wrong!
A 2-year-old female is brought to the physician by her mother who says her face turns blue when she cries. She also has trouble keeping up with her older brother when they play outside. An echocardiogram is obtained which reveals an anterosuperior displacement of the infundibular septum. The most important determinant of her prognosis is the
right ventricular hypertrophy
ventricular septal defect
Correct!
Wrong!
A 24-year-old female comes to the physician due tourinary frequency and burning with urination. She is diagnosed with a urinary tract infection and prescribed ciprofloxacin. The mechanism of action of ciprofloxacin is by
creation of transmembrane channels
inhibition of cell wall synthesis
inhibition of dihydrofolate reductase
inhibition of protein synthesis
Correct!
Wrong!
A 35-year-old male comes to the physician due towatery diarrhea of two weeks’ duration. He also has a low-grade fever, fatigue and weight loss of 5kg (11 lbs) over thepast month. Laboratory findings include a CD4+ T cell count 70 cells/mm³. To find the cause of his diarrhea, the next best step is a test involving
acid fast staining of the stool
cysts with multiple nuclei in the stool
silver staining of the stool
Correct!
Wrong!
A 30-year-old primigravid femaleat 16 weeks' gestation comes to the physician for a routine prenatal examination. She has no pre-existing medical conditions and thus far her pregnancy has been uncomplicated. She currently takes prenatal vitamins and iron supplements. Vitals reveal a blood pressure of 160/110 mm Hg. Urinalysis reveals 3+ proteinuria. The most likely cause of these findings is
Correct!
Wrong!
A 35-year-old male comes to the physician due to fatigue. He recently returned from a trip to Japan. Laboratoryresults are as follows:
Hemoglobin 9 g/dL
Mean corpuscular volume 108 fl
MCHC 33 g/dL
Mean corpuscular hemoglobin 35 pg
A peripheral blood smear is obtained which reveals enlarged red blood cells and hypersegmented neutrophils. These findings were most likely caused by
Correct!
Wrong!
A 55-year-oldfemale comes to the physician with a dry cough of three weeks’ duration. The cough is not associated with sputum or blood production and she is afebrile. She has a medical history of rheumatoid arthritis, peptic ulcer disease and hypertension for which is receiving treatment. The most likely cause of her chief complaint is
Correct!
Wrong!
A 35-year-old male comes to the physician due to fatigue. He recently returned from a trip to Japan. Laboratoryresults are as follows:
Hemoglobin 9 g/dL
Mean corpuscular volume 108 fl
MCHC 33 g/dL
Mean corpuscular hemoglobin 35 pg
A peripheral blood smear is obtained which reveals enlarged red blood cells and hypersegmented neutrophils. If these findings were caused by an infection, the most likely source of the infection is via
Correct!
Wrong!
A 60-year-old male with a past medical history of hyperlipidemia and hepatic dysfunction comes to the physician for a routine examination. He states that he has had difficulty initiating urination for the past seven months with an intermittent urine stream and urinary urgency. Vitals reveal a blood pressure of 150/90 mm Hg,a heart rate of 65/min, a temperature of 37.0°C (98.6°F) and a respiratory rate of 12/min. Digital rectal examination reveals diffuse enlargement of the prostate. The most appropriate pharmacologic treatment for this patient is most likely a drug that
activates central alpha-2 receptors
blocks alpha and beta receptors
blocks muscarinic receptors
inhibits 5-alpha reductase
selectively blocks alpha-1 receptors
Correct!
Wrong!
1 A 2-hour-old female who is born at 37 weeks' gestation has purple patches on her skin as well as hepatosplenomegalyand jaundice. A CT of the head is obtained which reveals periventricular calcifications. The most likely cause of these findings is also responsible for
heterophile negative mononucleosis
Correct!
Wrong!
A 50-year-old malewho is a known alcoholic is brought to the emergency department by police. He complains of a productive cough with thick, bloody sputum. Vitals reveal atemperature of 38°C (100.4 °F). Physical examination reveals dullness to percussion, increased tactile fremitus and decreased breath sounds over the right lung fields. A chest radiograph is obtained which reveals consolidation inthe right upper lobe. The most likely cause of these findings is a
gram-negative oxidase-negative bacillus
gram-positive oxidase-positive bacillus
gram-negative pleomorphic bacillus
gram-positive catalase-negative coccus
gram-positive catalase-positive coccus
Correct!
Wrong!
A 45-year-old male who has a BMI of 42 kg/m²undergoes a myocardial perfusion scintigraphy due to frequent chest pain during strenuous activities. An angiogram had earlierrevealed a 95% occlusion in the proximal segment of his left circumflex coronary artery. There were no changes in the othercoronary arteries. The most likely other finding in this patient is
inducible myocardial ischemia in the anterior segment of the left ventricle
inducible myocardial ischemia in the anteroseptal segments of the left ventricle
inducible myocardial ischemia in the inferior segments of the right ventricle
inducible myocardial ischemia in the inferolateral segment of the left ventricle
inducible myocardial ischemia in the septal segments of the left ventricle
Correct!
Wrong!
A 2-year-old female is brought to the physician by her mother who says her face turns blue when she cries. She also has trouble keeping up with her older brother when they play outside. An echocardiogram is obtained which reveals an anterosuperior displacement of the infundibular septum. The most likely diagnosis is
transposition of the great vessels
Correct!
Wrong!
A 45-year-old female comes to the physician with joint pain, swelling and morning stiffness which improves with use. She also reports weight loss of 3 kg (6.6 lbs). Laboratory tests reveals the presence of serum rheumatoid factor.The most likely other finding in this patient is
anti-acetylcholine receptor antibodies
anti-centromere antibodies
anti-cyclic citrullinated peptide antibodies
anti-smooth muscle antibodies
anti-U1 ribonucleoprotein antibodies
Correct!
Wrong!
A 2-year-oldmaleis brought to the physician due to mental retardation. Physical examination reveals a single palmar crease, flat face and prominent epicanthal folds. The most likely cause of these findings is
Robertsonian translocation
Correct!
Wrong!
A 40-year-old male is brought to the emergency department due to progressive memory loss, confusion, and urinary incontinence.Laboratory studies reveala CD4 cell count of 25/mm³. A MRI reveals moderate brain atrophy. Although the patient is admitted for treatment he eventually dies of disseminated aspergillosis. Microscopic examination of an autopsy specimen from hisbrain shows multifocal lymphohistiocytic infiltrates with numerous microglial nodules and scattered multinucleated giant cells. His histologic and MRI findings were most likely caused by
progressive multifocal leukoencephalopathy
Correct!
Wrong!
A 25-day-old male is brought to the physician due to seizures, rigidityand frequent viral infections. Physical examination reveals a neonate with cyanosisin the lower extremities. The most likely cause of these findings is a
defect in the IL-2R gamma chain
defect in the lysosomal trafficking regulation gene
defect in the tyrosinase kinase gene
deletion in chromosome 22q11.2
mutation in the STAT3 gene
Correct!
Wrong!
A 2-week-oldmale is brought to the physician by his mother due to labored breathing for the past day. She had a home delivery which she reports as uneventful but sayshe developed "pink-eye" after thefirst week. Vitals reveal a respiratory rate of 40/min. Physical examination reveals bilateral inspiratory crackles and faint wheezingin both lungs. Laboratory studies reveal a leukocyte count of 15,000/mm³ with 10%
Correct!
Wrong!
A 45-year-old maleis broughtto the emergency department by the police who found him wandering around a park at midnight. Physical examination reveals bilateral hand tremors. Laboratory tests reveal elevated serum gamma-glutamyltransferase. Thirty hours after he is admitted to the hospital he developsgeneralized seizures. The most appropriate treatment for this patient’s seizures is
Correct!
Wrong!
A 50-year-old male is brought to the emergency department due to an acute onset chest pain that radiates to his jaw. An ECG revealsST segment elevation in leads II, III and aVF. He undergoes percutaneous coronary intervention with stenting without any complications. The patient is discharged from the hospital three days later withaspirin and clopidogrel. He returns to the emergency department eight weeks later due to recurrent chest pain which he describes as a sharp pain that worsens when he lies flat. The pain does not radiate or improve with nitroglycerin tablets. Vitals reveal a blood pressure of 135/87 mm Hg, a heart rate of 84/min, a temperature of 38.0°C (100.5°F) and a respiratory rate of 12/min. Oxygen saturation is 98% on room air. Physical examination revealsa harsh three component extra heart sound heard best at the left lower sternal border. An ECG is obtained which reveals diffuse ST elevations. The most likely cause of the current findings is
Correct!
Wrong!
Subscribe to see your results
FREE USMLE Practice Exam
I got %%score%% of %%total%% right
%%description%%
Loading...
What was your score? Are you ready to take the USMLE Step 1 exam?
What is the USMLE?
The USMLE Step 1 Exam is administered over the course of one day consisting seven 60-minute sessions. Each session will have 40 or fewer questions. The following topics are found on this exam:
- Anatomy
- Behavioral Sciences
- Biochemistry
- Biostatistics and Epidemiology
- Microbiology
- Pathology
- Pharmacology
- Physiology
In addition to the above topics, the USMLE Step 1 Exam also covers interdisciplinary areas related to the following:
- Aging
- Genetics
- Immunology
- Molecular and Cell Biology
- Nutrition
Smash USMLE provides a USMLE Step 1 Prep Courses and Qbanks which have 2,000+ USMLE Step 1 practice questions. These questions are written in the same format found on the exam and have detailed explanations like the ones you’ll see here. Each of the categories found on the exam is covered by the Smash USMLE question bank and will provide you with hands-on experience for what to expect on the testing day. Want more practice? Compare the best USMLE Step 1 review courses here.
-
Tweet -
Share
0 -
Pocket -
VKontakte - 1
- Войдите, чтобы голос был засчитан
Мне сложно придумать, с чего начать свой рассказ, так как на достижение этой цели ушло почти 4 года, а на то, чтобы решиться поставить себе такую цель у меня ушла почти вся жизнь.

Предыстория
История с поступлением в американскую резидентуру началась одним летним вечером, когда муж как бы невзначай спросил меня: “А не хочешь ли ты переехать в США?” Я немного напряглась, так как знаю, что в нашей семье от слов до дела доходит очень быстро. Например однажды он спросил, как я смотрю на переезд из Ростовской области в Москву, и через пол года мы уже обустраивались в однокомнатной квартирке в Новокосино. Еще как-то раз он спросил, не хотела бы я пробежать полумарафон, оказалось, что хотела и, внезапно через несколько месяцев я обнаружила себя на финише “Осеннего грома”. А однажды он поинтересовался, не хотела бы я сменить задолбавшую меня работу в фармкомпании на работу в сфере IT. И угадайте, что произошло? Да, я человек с медицинским образованием, научилась составлять семантические ядра, заниматься аналитикой посещаемости сайтов и устроилась в SEO-компанию. Как вы поняли, в нашей команде муж — дерзкий идейный
вдохновитель, а я — склонный к авантюризму исполнитель. И вот, как раз когда я только вошла во вкус на новой работе, был задан этот исторический вопрос про переезд в США.
Не буду томить описанием всех своих сомнений, сразу скажу, что в итоге я согласилась, но на принятие этого решения у меня ушло около двух месяцев. Все это время главным вопросом для меня было то, чем я могу там заниматься, кроме как сидеть дома. Изучив рынок, я поняла, что без американского образования я смогу отлично вписаться только в ряды официантов или бездомных. Получать американское образование было слишком дорого и мне оставалось только одно: подтверждать уже имеющийся у меня диплом — медицинский.
Надо сказать, что с медициной у меня “все сложно”. Мечта стать патологоанатомом появилась у меня лет в 13 под влиянием сериала “Секретные материалы”. Мне никогда не было интересно лечить, скорее хотелось изучать “что внутри” и разгадывать тайны нашей маленькой плотской вселенной. Вопросов на тему профориентации с тех пор у меня не возникало и я, как по накатанной, пошла по ступеням медицинского образования. Но где-то по пути я несколько раз свернула не туда и выпустилась из университета врачом-гастроэнтерологом. С первого рабочего дня я всеми чакрами чувствовала, что это не мое, и ради безопасности пациентов ушла из медицины вообще. Вот такая краткая предыстория и сказ о том, как я сбилась с пути и забыла о своем предназначении.
Мотивы
И вот, переезд в другую страну! Самый частый вопрос, который мне задают на эту тему: “Почему Штаты? И зачем вообще куда-то переезжать?” Первое время я пыталась говорить красивыми словами, сыпала экономическими терминами, выдумывала какие-то истории о “невероятных карьерных возможностях”. Но потом мне это надоело, и я стала отвечать честно: “Мне просто интересно!”. На момент постановки цели я ни разу не была в Штатах. Но мы с мужем много путешествовали по миру и я понимала, что с нашим характером мы сможем прижиться где угодно. А уж пара программист + врач — это просто формула успеха, поэтому мы решили, что игра стоит свеч!
Сейчас я думаю, что определяющим фактором в принятии решения для меня все-таки была возможность вспомнить о своей мечте стать патологом, о том, к чему у меня действительно лежит душа и в чем, возможно, мое предназначение. Моя основная мотивация была в том, чтобы воплотить все это в жизнь так, как я никогда бы не смогла сделать это в своей родной стране.
Постановка цели
Итак, однажды пришло время формировать цель, выстраивать какую-то последовательность действий. И здесь я столкнулась с первой сложностью. Оказалось, что подтверждение медицинского диплома в США — не такая уж популярная тема в России и знают о ней только избранные. У меня не было никаких знакомых или даже знакомых знакомых, которые хотя бы краем уха слышали об этом. В интернете, даже на официальных сайтах, информация была запутанной и вызывала только больше вопросов — это был чистый хаос! Я поняла только то, что моя ординатура в Штатах не зачитывается и специализацию в любом случае нужно получать заново. Для этого нужно сдать какие-то нереально сложные и дорогие экзамены под названием USMLE, а потом пройти какой-то супер-конкурентный отбор в резидентуру (это аналог нашей ординатуры). Но с чего начать, как готовиться и кому платить было неясно, все это приходилось выковыривать из недр интернета по маленьким кусочкам.
И, когда я уже начала впадать в панику из-за нагромождения информации, мои знакомые бегуны посоветовали попробовать поставить себе цель на SmartProgress. Они обычно там ставили себе цели на забеги и вели дневник подготовки. Мне структура сервиса подходила идеально, и я решила постепенно составлять этапы, которые должны привести меня к желаемому. Так родился мой блог. Я тогда еще не знала, какие тесные отношения у меня с ним сложатся, сколько слез я пролью, описывая все свои неудачи, сколько поддержки я там найду и сколько полезной информации там накопится для следующих поколений сдающих USMLE.
Вкратце этапы цели выглядели так:
- Сдать 3 экзамена ——> получить сертификат о том, что мой диплом подтвержден
- Пройти практику в США ——> получить 3 рекомендательных письма от американских
врачей (это обязательное требование для поступления в резидентуру) - Подать документы в Матч (это процесс отбора кандидатов в резидентуру) и пройти
собеседования на позицию резидента-патолога, если вдруг меня кто-то вообще
пригласит.
Таймлайн у меня был растянут на 2 года, я думала, что смогу в него уложиться, наивная. Все выглядело просто и местами понятно, поэтому поначалу я еще не осознавала, в какую серьезную игру я начинаю играть и каких страшных жертв мне это будет стоить.
Жертвы. Ой, точнее “Ресурсы”.
Первой жертвой стала работа. Я поняла, что не смогу совмещать ее с подготовкой к
экзаменам. Почему? Да потому что среднее время подготовки к первому экзамену равняется 12 месяцам! Мне не хотелось терять столько времени и я решила готовиться фулл-тайм. Я садилась за учебники где-то в 9 утра и вставала в 6 вечера, то есть у меня был полноценный рабочий день. Но даже с таким режимом на подготовку к первому экзамену у меня ушло 18(!) месяцев вместо запланированных 10. Из-за этого мне пришлось 2 раза переносить дату экзамена, чтобы доползти до своих целевых баллов.
И теперь уже пришлось жертвовать деньгами. Надо сказать, что USMLE — недешевое
удовольствие, один экзамен стоит в среднем $1000. А за то, чтобы перенести его во второй раз мне пришлось заново оплачивать полную стоимость. Но это была капля в море всех последующих трат. Итоговая сумма всех затрат перевалила за $30.000, то есть 2 млн руб. Полную детализацию этих расходов можно посмотреть на странице цели, но там я не учитывала траты во время поездок в Штаты, так что реальная сумма все же значительно выше. Откуда я брала деньги? Тоже очень частый вопрос. Отвечаю: на это ушли все сбережения, отложенные на ипотеку. А когда они кончились, вся работа по спонсированию этого безумного мероприятия легла на плечи моего несчастного мужа, который уже потихоньку начинал жалеть, что когда-то задал мне этот судьбоносный вопрос.
Когда меня спрашивают, как решиться или как понять, что ты осилишь USMLE, я всегда отвечаю одинаково. Первое: оцените свои финансы, без них эту цель не завершить, это вообще основное топливо всего процесса. Без $ вы не сможете даже зарегистрировать личный кабинет для регистрации на экзамен. Второе: оцените свой ресурс времени, особенно если вы вынуждены работать или у вас есть маленькие дети, это может стать непосильной задачей, хотя есть масса примеров, когда даже с такими условиями люди сдавали на выдающиеся баллы. И третье: четко поймите, для чего вам это нужно. Вы должны создать себе настолько сильную внутреннюю мотивацию, которая протащит вас через годы морального истощения и финансовой нестабильности, кои являются непременным атрибутом дороги к резидентуре.
Экзамены
Экзамены USMLE считаются одними из самых сложных экзаменов в мире. Этих экзаменов всего 4: Step1, Step2 CK, Step2 CS и Step3. Первые три обязательны для подтверждения медицинского диплома, а последний можно сдавать уже в резидентуре. Американские студенты сдают их во время обучения в мед школе, для них это обычная проверка полученных знаний. Для меня же это стало проверкой на прочность, так как на момент начала подготовки я не была студенткой уже 5 лет и не помнила, ни того, что проходила в университете, ни того, как нужно продуктивно учиться. Тем более на неродном языке!
Почему эти экзамены такие сложные? Step1 и Step2 Clinical Knowledge сдаются в виде
тестов, которые длятся 9 и 8 часов соответственно. Представьте себе тест, который длится 9 часов. Даже если бы нужно было просто складывать двузначные числа все это время, то и в этом случае было бы тяжко, но тесты устроены гораздо сложнее, порой в них даже сам вопрос является неочевидным и его нужно вычислять с помощью дедукции, а уж ответы больше похожи на заклинания из некрономикона, особенно если это связано с биохимией. Это не такие тесты, ответы к которым можно просто заранее вызубрить и ждать, когда тебе попадется выученный вопрос. Нет, содержание тестов держится в строжайшем секрете, они регулярно обновляются и с каждым годом становятся все сложнее.
Step2 Clinical Skills отличается от остальных экзаменов, он практический. Ты должен за
ограниченное время осмотреть 12 пациентов, которых играют актеры, поставить им диагноз, проконсультировать и заполнить историю болезни. Потом твой перфоманс оценивают по трем параметрам: разговорный английский, качество медосмотра и навыки общения с пациентом, которым в российских медвузах учат крайне условно. Да, очень важно создать атмосферу доверия, вовремя успокоить пациента и сказать “Я понимаю, через что вы проходите, и сделаю все, что могу, чтобы помочь вам”. Нужно объяснять каждое свое действие, спрашивать разрешения прежде чем коснуться тела пациента и обязательно мыть руки до и после этого. Помимо всего этого этикета нужно еще успеть понять, что же с пациентом не так.
Самый последний Step3 — еще один тест, но он длится не несколько часов, а целых два дня. С перерывом на сон конечно. Теперь вы понимаете, что мне предстояло?
Трудности подготовки
Все три года моей подготовки (именно столько у меня ушло на сдачу всех экзаменов USMLE) можно описать двумя словами: “долго” и “мучительно”. Нет, иногда я конечно получала какое-то удовольствие от учебы, от того, что узнаю что-то новое, что начинаю разбираться в каких-то сложных и уникальных вещах, качество получаемых мной знаний было на порядок выше, чем то, чему я училась в университете. Но вы только представьте, как это, 3 года подряд каждый божий день заниматься самообразованием, вкладывать в него все свои деньги, жертвовать другими своими интересами, и все это без каких-либо гарантий, что это вообще выстрелит. Атмосфера ненадежности и неуверенности усугублялась еще и тем, что сроки все время сдвигались, подготовка давалась мне сложнее, чем я рассчитывала, я никак не могла дойти до своих целевых баллов. В итоге, после 18 месяцев подготовки к первому
степу, я решила, что пора это прекращать и идти сдавать, как есть.
Сдала я плохо. Мой балл был ниже среднего, что-то типа тройки с минусом в мире USMLE. Такой результат не был для меня неожиданным, но он все равно сильно пошатнул мою уверенность в себе. Мне всегда казалось, что я сообразительная и что у меня отличная память, но либо я ошибалась, либо экзамен был совсем не об этом. В любом случае тут я поняла, что нужно менять свое отношение к подготовке и переходить из режима “авантюра” в режим “все серьезно”. Я решила взять реванш на втором экзамене.
Готовилась я к нему 6 месяцев, на этот раз четко уложившись в срок. И это была совсем другая подготовка. Я перестала заниматься дома и стала ходить в Тургеневскую библиотеку. Приходила к открытию и уходила под вечер. Учебники, тесты, бесконечные флеш-карты, несколько кофейных стаканов на столе и мирное библиотечное шуршание — так прошли те пол года. И проверочные тесты показывали значительный прогресс. Я была очень воодушевлена и полна надежд.
Как же было горько потом узнать, что сдала я гораздо хуже всех прогнозов! Балл за второй экзамен оказался всего лишь чуть выше предыдущего. И мне сложно описать, что я почувствовала, когда увидела эти цифры на экране. Даже сейчас, когда я это пишу, у меня наворачиваются слезы. В тот момент во мне как будто что-то потухло и внутри начала расползаться черная дыра. Никогда в жизни я столько не работала и не вкладывала столько сил во что-то, это был уникальный для моей жизни случай полной самоотдачи и напряжения всех своих возможностей. И что я получила в результате!? Балл ниже среднего, о котором большинство людей даже стесняется рассказывать!
У меня началась депрессия. Несмотря на то, что я уже зарегистрировалась на третий
экзамен и начала оформление на практику в Америке, я не хотела ничего этого делать, у меня не было на это энергии. Мне стало казаться, что эти баллы оценивают мою личность и что это не они, а я — “ниже среднего”. Плюс ко всему с такими баллами шансов попасть в резидентуру у меня почти не оставалось, так как скоры — ключевой фактор при отборе кандидатов.
В таком состоянии я пробыла около месяца. Из режима “все серьезно” я перешла в режим “все тлен”. Мой бедный муж наблюдал за моим отчаянием и помогал, как мог. Для него эта история тоже была большим стрессом и стоила ему многих жертв.
Мой катарсис

Но после ночи всегда приходит рассвет. Дав себе время на оценку ситуации, не принуждая себя как можно быстрее что-то решать, я потихоньку начала возвращаться к адекватному восприятию происходящего. К тому моменту я занималась USMLE уже 2 года, самые сложные экзамены я сдала и мне оставался только один самый “простой”. Я решила, что если я не попытаюсь его сдать, то просто потеряю остатки уважения к себе и буду всю жизнь думать о том, какую возможность упустила.
На подготовку к практическому экзамену я потратила чуть больше месяца. Это была очень безрадостная подготовка ради галочки, весь мой энтузиазм к тому моменту совершенно потух. Мне просто хотелось скорее дойти до конца. Вы когда-нибудь смотрели марафон? Там всегда есть люди, которые уже почти добежали до финиша, они видят его перед собой, но не могут ступить и шагу, потому что они окончательно выдохлись. Вот так я себя чувствовала. Но вы наверное видели и то, как таких уставших бегунов подхватывают пробегающие мимо более энергичные ребята и просто доносят их до финиша. Таким человеком для меня стал мой стади-партнер. Этот человек наверное даже не знает, как он мне помог тогда, но если он читает, то наверное поймет, что я говорю именно о нем.
Результат третьего экзамена я ждала почти 2 месяца. Это время я решила не терять зря и устроилась на практику в Штатах. Мне же нужно было где-то достать 3 рекомендательных письма. Я устроилась на 3 недели в отделение Патологии в одном госпитале недалеко от Чикаго и еще на 3 недели в частной патологической лаборатории в пригороде Атланты. И эти 6 недель перевернули мой мир!
Меня удивило, как ко мне относились врачи и весь персонал больницы: со мной общались на равных, им интересно было меня учить и я ни разу не почувствовала себя чужой. Когда я ходила на собрания врачей, мой аттендинг мог обратиться к спикеру и сказать: “Доктор, у нас здесь сегодня студент, не могли вы рассказать ему поподробнее о том лечении, которое вы предлагаете?” И этот доктор, такой весь солидный, поворачивался ко мне и спокойно, даже с энтузиазмом объяснял детали терапии!
Первую неделю я просто изучала теорию и наблюдала, как работают ассистенты патолога, которые вырезают из органов кусочки ткани для их подготовки к микроскопическому исследованию. Затем настал час, когда мне дали в руки скальпель и доверили самой препарировать плаценту. В тот самый момент со мной произошло что-то очень важное. Я почувствовала, что наконец нашла себя. Я была в том месте, в котором я должна быть, и делала то, для чего я родилась! Это звучит ужасно пафосно, но для меня это было чудесным открытием, этаким божественным лучом света, который озарил мне весь последующий путь. В тот день я ехала домой, заливаясь слезами счастья и благодарности. В тот день вся эта история наконец обрела для меня смысл.
Безумству храбрых поём мы песню!
К концу практики я узнала, что сдала третий экзамен.Это окончательно убедило меня в том, что удача на моей стороне и нужно ковать пока горячо. Да, удача мне была очень нужна! С моими баллами, давнишним годом выпуска, большим перерывом в работе и отсутствием грин карты я была не самым конкурентоспособным кандидатом. Чтобы хоть как-то украсить свое резюме я решила сдать последний,четвертый, экзамен, который обычно сдают уже в резидентуре.
Когда пришел результат, то балл меня уже совершенно не волновал, я стала к этому
абсолютно пуленепробиваема. Тогда я уже познала дзен и понимала, что меня определяют не эти цифры, а то, насколько я уверена в том, что иду своей дорогой. Эта дорога определенно была моей и я была решительно настроена дойти до конца.
И вот, я подала свою заявку, над которой я работала 3 долгих года! Процесс отбора кандидатов — это дело крайне серьезное и сложносочиненное. Ты загружаешь все свои документы на портал и рассылаешь их во все программы, куда хочешь поступить. Это удовольствие естественно не бесплатное, каждая заявка обходится в $26. Я подала свое резюме в 133 программы по Патологии, то есть почти во все. Затем каждая программа отфильтровывает из сотен кандидатов те единицы, которые затем приглашает на интервью. В моей специальности в среднем это 8-10 человек на место. Сезон интервью длится с октября по февраль и затем начинается “лотерея” по распределению мест под названием Match. Результаты приходят всем в один день — в третий понедельник марта.
Со своими данными я не рассчитывала на интервью. Вся статистика говорила о том, что кандидатов вроде меня могут пригласить только по ошибке, так что я планировала найти временную работу, а потом попробовать поучаствовать в борьбе за оставшиеся после Матча места. Каким же было мое удивление, когда всего через два дня после отправки документов мне пришло первое приглашение! Ребята, счастливее меня могли быть только шахтеры, которых вытащили из замурованной шахты!
Но это было только начало! В итоге меня пригласили на целых 4 интервью, и я провела в Америке 2 месяца, катаясь по разным штатам и больницам, чтобы пройти в них собеседование. О том, как я готовилась и как проходили эти интервью, я в красках
рассказывала на страничке своей цели на Смартпрогресс. Меня тогда поддерживало очень много людей и я безумно благодарна за то вдохновение, которое мне эта поддержка давала. Все то время мне казалось, что я внутри какого-то фильма, все вокруг было нереальным, слишком хорошим, чтобы быть правдой.
Мой сезон интервью закончился в декабре. Оставалось только ждать марта, когда будут объявлены результаты. Три месяца ожидания! Никогда время не тянулось ТАК ДОЛГО! Я старалась не сидеть без дела и писала любовные письма в программу, в которую я хотела попасть больше всего. Но все равно еще оставались шансы, что я не попаду вообще никуда. Об этом я старалась не думать и не строила планов на случай неудачи.
Вы наверное уже поняли, что никаких запасных планов мне не понадобилось. У меня все получилось! И сматчилась я именно в ту программу, которая мне понравилась больше всех! Момент получения результатов был наверное самым сильным эмоциональным переживанием в моей жизни. У меня было ощущение, что я добилась чего-то за гранью своих возможностей, чего-то, о чем я даже и не смела мечтать.Большую часть жизни я считала, что я недостаточно хороша для каких-то серьезных достижений, у меня никогда не было честолюбивых амбиций или особых способностей. Что у меня было, так это тяга к приключениям и какой-то внутренний компас, который подсказывал мне, где эти приключения искать.

Вся эта история очень изменила меня. Я научилась воспринимать неудачи, как часть пути, а не как его конец. Я поняла, что никакие цифры и баллы не могут измерить объем моей личности. Выяснилось, что даже когда кажется, что шансов нет, один все-таки может найтись, нужно только хорошенько поискать. Еще нужна капелька бесстрашия. Попробуйте разочек рискнуть, и вы увидите, как много неожиданных возможностей откроется перед вами. Посмотрите фильм “Всегда говори Да”. О, я смотрела его миллион раз! Он очень близок мне по духу. Может быть и вас он вдохновит согласиться на что-то, от чего вы раньше отказывались. А может быть таким вдохновением для вас станет моя история.
Сейчас моя цель на смартпрогресс уже на этапе завершения. Мне осталось только оформить некоторые документы и совсем скоро я смогу начать идти к новой цели, решать еще более сложные задачи. Вы можете присоединиться и следить за всеми этими приключениями на моей страничке. Впереди у меня 4 года обучения в резидентуре в Портленде, штат Орегон, а дальше… дальше, целая жизнь, полная непредсказуемости!
-
Tweet -
Share
0 -
Pocket -
VKontakte - 1
- Войдите, чтобы голос был засчитан
The following three USMLE Step 1 sample questions from TrueLearn’s SmartBank test some of the high-yield material you’re sure to see on exam day. Each question is followed by an authoritative answer explanation, complete with rich visuals, a focused Bottom Line statement, and supporting references (including page numbers from First Aid for the USMLE Step 1). Finally, each question also includes a unique TrueLearn Insight.
TrueLearn Insights are where our expert author team provides Step-wise strategies and tables to help you master the exam. Inspired by our authors’ own experience studying and tutoring for Step 1, they address common student struggles through detailed insider advice. As a supplement to our thorough answer explanations, TrueLearn Insights provide added value not available from any other USMLE question bank.
For thousands of other high-yield practice questions, along with exam-focused answer explanations, summary tables, figures, Bottom Line statements, and references—plus more exclusive TrueLearn Insights—order a free trial today.
First Step 1 Sample Question: Anemia
A 65-year-old woman presents to the office with generalized fatigue for the last 4 months. She used to walk 1 mile each evening but now gets tired after 1-2 blocks. She has a history of Crohn disease and hypertension for which she receives appropriate medications. She is married and lives with her husband. She eats a balanced diet that includes chicken, fish, pork, fruits, and vegetables. She rarely drinks alcohol and denies tobacco use. Her vital signs are within normal limits. A physical examination is unremarkable. Laboratory studies show the following:
- Hemoglobin: 9.8 g/dL
- Hematocrit: 32%
- Mean corpuscular volume: 110 μm3
- Platelets: 180,000/mm3
- Leukocytes: 5200/mm3
The patient is prescribed oral vitamin B12 supplementation and advised to return to the clinic for follow-up in 1 month. Laboratory studies performed at that time show persistent anemia with a serum hemoglobin of 9.5 g/dL. Which of the following is the most likely cause of this patient’s anemia?
The patient is prescribed oral vitamin B12 supplementation and advised to return to the clinic for follow-up in 1 month. Laboratory studies performed at that time show persistent anemia with a serum hemoglobin of 9.5 g/dL. Which of the following is the most likely cause of this patient’s anemia?
A. Chronic blood loss
B. Complement mediated destruction of red blood cells
C. Decreased release of iron from macrophages due to chronic inflammation
D. Dietary deficiency of folate
E. Impaired intestinal absorption of vitamin B12
F. Pancreatic insufficiency
Answer
| Vitamin B12 (Cobalamin) Deficiency | |
| Etiology | Dietary deficiency (eg, vegans) Intestinal malabsorption (eg, Crohn disease) Lack of intrinsic factor (pernicious anemia) Post gastrectomyPost gastric bypass surgery Pancreatic insufficiencyDiphyllobothrium latum (fish tapeworm) |
| Presentation | Anemia often takes years to develop, given the large hepatic stores of vitamin B12Fatigue and generalized weakness Decreased exercise tolerance Neurologic symptoms → subacute combined degeneration Dorsal columns → defects in proprioception; positive Romberg sign Spinocerebellar tract → ataxia Lateral corticospinal tract → motor weakness |
| Laboratory Findings | Macrocytic anemia (mean corpuscular volume > 100 μm3) Hypersegmented neutrophils seen on peripheral blood smear ↑ homocysteine ↑ methylmalonic acid |
When approaching anemia questions on the USMLE, start by evaluating the mean corpuscular volume (MCV) as this will allow one to narrow down the list of possible answers. Here, the patient has an MCV > 100 μm3, pointing toward a macrocytic anemia. Common causes of macrocytic anemia include:
- Vitamin B12 deficiency
- Folate deficiency
- Orotic aciduria
- Alcoholism
- Liver disease
After evaluating the MCV, possible correct answers include dietary folate deficiency and impaired intestinal absorption of vitamin B12. Although this patient’s anemia did not improve with supplementation with vitamin B12, that does not rule out vitamin B12 deficiency as a cause of her anemia. This is because the absorption of vitamin B12 requires several key aspects, including:
- Adequate dietary intake of vitamin B12
- Binding of B12 with intrinsic factor (produced by parietal cells within the gastric mucosa)
- Successful absorption of vitamin B12 in the small intestine (particularly at the ileum)
Vitamin B12 deficiency can develop if any of these steps are impaired. In this case, the patient’s history of Crohn disease should raise suspicion that impaired intestinal absorption of vitamin B12 is the cause of her anemia. Crohn disease can occur anywhere within the gastrointestinal tract, except for the rectum, but most commonly involves the ileum and small intestine. As a result of ileal damage, patients may have impaired absorption of vitamin B12. In these cases, oral supplementation with vitamin B12 will be ineffective as the ileal damage will still prevent sufficient absorption. A similar finding would be expected in cases where patients are lacking intrinsic factor (eg, pernicious anemia, post gastrectomy).
Historically, the Schilling test would have been used to assess whether vitamin B12 deficiency was due to a dietary deficiency or malabsorption. This test involved four distinct phases:
- Phase 1: The patient is given radiolabeled vitamin B12 to drink or eat. Several hours later, urine is collected and examined for the presence of radiolabeled vitamin B12. The presence of radiolabeled vitamin B12 in the urine implies that the patient is able to absorb vitamin B12 and, thus, is suggestive of a dietary deficiency as the underlying etiology.
- Phase 2: If radiolabeled vitamin B12 did not appear in the urine, then the patient is given another dose of radiolabeled vitamin B12 and intrinsic factor. If radiolabeled vitamin B12 now appears in the urine, then it suggests a lack of intrinsic factor as the underlying etiology.
- Phase 3: The patient is given radiolabeled vitamin B12 and antibiotics. If radiolabeled vitamin B12 now appears in the urine, then bacterial overgrowth is the likely underlying etiology.
- Phase 4: The patient is given radiolabeled vitamin B12 and pancreatic enzymes. If radiolabeled vitamin B12 now appears in the urine, then pancreatic insufficiency is the likely etiology. If radiolabeled vitamin B12 is still not in the urine, then this is suggestive of ileal disease.
The Schilling test is no longer routinely used in the clinical setting. However, it may still appear on the USMLE.
Did you get it right? The correct answer was E.
Further Explanation
Answer A: Chronic blood loss can result in iron deficiency anemia. However, iron deficiency anemia is a form of microcytic anemia and would have an MCV < 80 μm3. Iron deficiency anemia should not be considered in a patient who has evidence of macrocytic anemia.
Answer B: Complement mediated destruction of red blood cells is the pathophysiology of paroxysmal nocturnal hemoglobinuria, which is a form of hemolytic anemia and thus would be a normocytic anemia. On laboratory studies, normocytic anemias have an MCV of 80-100 μm3.
Answer C: Anemia of chronic disease occurs as chronic inflammation impairs the release of iron from macrophages and decreases the intestinal absorption of iron. It is most commonly seen with conditions such as lupus, rheumatoid arthritis, and chronic kidney disease. Here, anemia of chronic disease should be eliminated as a possible answer because it typically presents as either a normocytic (most common) or microcytic anemia.
Answer D: Dietary deficiency of folate can result in a macrocytic anemia. However, folate is found in leafy green vegetables. Given that this patient eats a balanced diet with fruits and vegetables, folate deficiency is much less likely than vitamin B12 deficiency secondary to deficient intestinal absorption.
Answer F: Pancreatic insufficiency can result in either a normocytic anemia (due to vitamin E deficiency) or a macrocytic anemia (due to vitamin B12 deficiency). If pancreatic insufficiency were the cause of this patient’s vitamin B12 deficiency, than oral supplementation would not be expected to improve the anemia. However, this patient has no underlying history that would suggest she has pancreatic insufficiency. Causes of pancreatic insufficiency include chronic pancreatitis (often due to alcoholism and recurrent episodes of acute pancreatitis) and cystic fibrosis. Given her history of Crohn disease, impaired intestinal absorption of vitamin B12 is much more likely.
Bottom Line: Vitamin B12 deficiency can be seen in patients with Crohn disease due to impaired intestinal absorption of vitamin B12. In these cases, oral supplementation with vitamin B12 will not result in an improvement of their anemia or symptoms.
TrueLearn Insight
Make sure that you are comfortable differentiating among the different types of vitamin deficiency that can result in anemia. These topics are frequently tested together on the USMLE.
| Vitamin Deficiencies That Can Cause Anemia | ||||
| Vitamin B12 Deficiency | Folate Deficiency | Vitamin E Deficiency | Vitamin B6 Deficiency | |
| Mean Corpuscular Volume | > 100 μm3(macrocytic) | > 100 μm3(macrocytic) | 80-100 μm3(normocytic) | < 80 μm3(microcytic) |
| Etiology | Dietary deficiency (vegans) Pernicious anemia Post gastrectomy Post gastric bypass surgery Pancreatic insufficiency Impaired intestinal absorption (eg, Crohn disease) |
Malnutrition (alcoholics) Malabsorption Medications Methotrexate Trimethoprim PhenytoinIncreased metabolic demand Pregnancy Chronic hemolytic anemia |
Deficiency due to impaired absorption of fat-soluble vitamins (Pancreatic insufficiency, Biliary disease)
Vitamin E is an antioxidant → deficiency results in hemolytic anemia due to oxidative damage to red blood cells |
Medications (Isoniazid Oral contraceptives) |
| Clinical Features | Anemia takes years to develop due to large hepatic storage poolNeurologic symptoms | Anemia develops much sooner compared with vitamin B12 deficiencyNo neurologic symptoms | Neurologic symptoms similar to vitamin B12 deficiency | Peripheral neuropathy |
| Diagnostic Findings | Hypersegmented neutrophils ↑ homocysteine ↑ methylmalonic acid ↓ reticulocytes |
Hypersegmented neutrophils ↑ homocysteine Normal methylmalonic acid ↓ reticulocytes |
Findings consistent with hemolytic anemias ↑ lactate dehydrogenase ↑ reticulocytes ↑ total bilirubin ↓ haptoglobin |
Findings consistent with sideroblastic anemiaerythrocyte basophilic stippling ringed sideroblasts |
Second Sample Question: Hydrochlorothiazide Mechanism Of Action
A 57-year-old African American man comes to the office for follow-up regarding elevated blood pressures. Two months prior, the patient was diagnosed with hypertension due to an elevated blood pressure at multiple office visits. Since then, he has attempted to manage his blood pressure with dietary changes and exercise. Despite a 2.3-kg (5-lb) weight loss during this time, his blood pressure is 150/90 mm Hg on arrival and 152/88 mm Hg on repeat 10 minutes later. He has been tracking his blood pressure at home and notes that his systolic blood pressure ranges between 140 and 160 mm Hg. Given his persistent hypertension, pharmacologic intervention is initiated. Six weeks later, the patient returns to the clinic for follow-up evaluation. He notes that his blood pressures have improved, and his systolic blood pressure now ranges between 125 and 135 mm Hg. Serum laboratory studies are ordered and show the following:
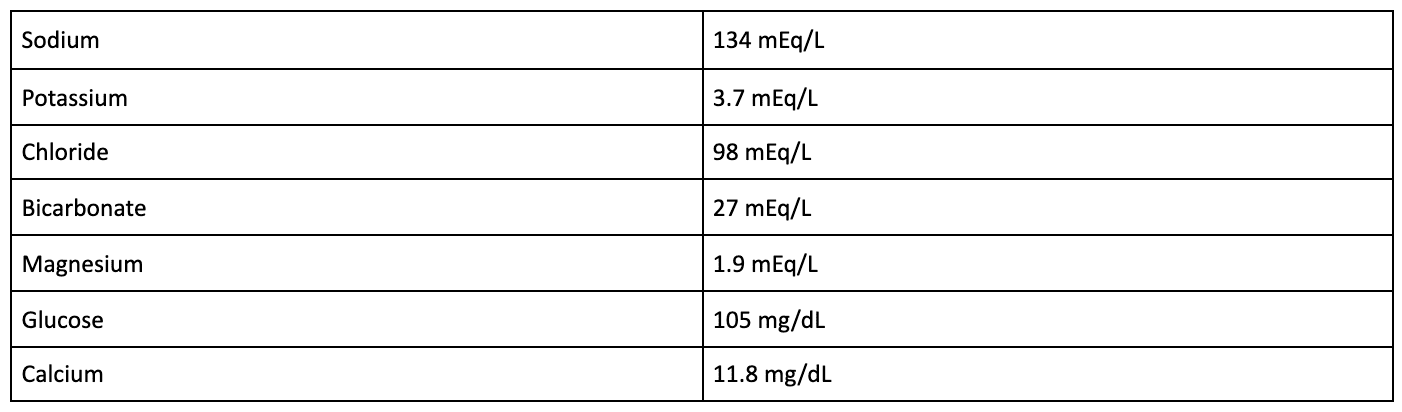
Which of the following best describes the mechanism of action of the pharmacologic agent most likely responsible for this patient’s laboratory findings?
- Blockage of voltage-dependent calcium channels in vascular smooth muscle
- Decreased production of angiotensin II
- Decreased renin secretion
- Increased cGMP-mediated arterial dilation
- Inhibition of sodium chloride reabsorption in the distal convoluted tubule
Explanation
The correct answer is: E
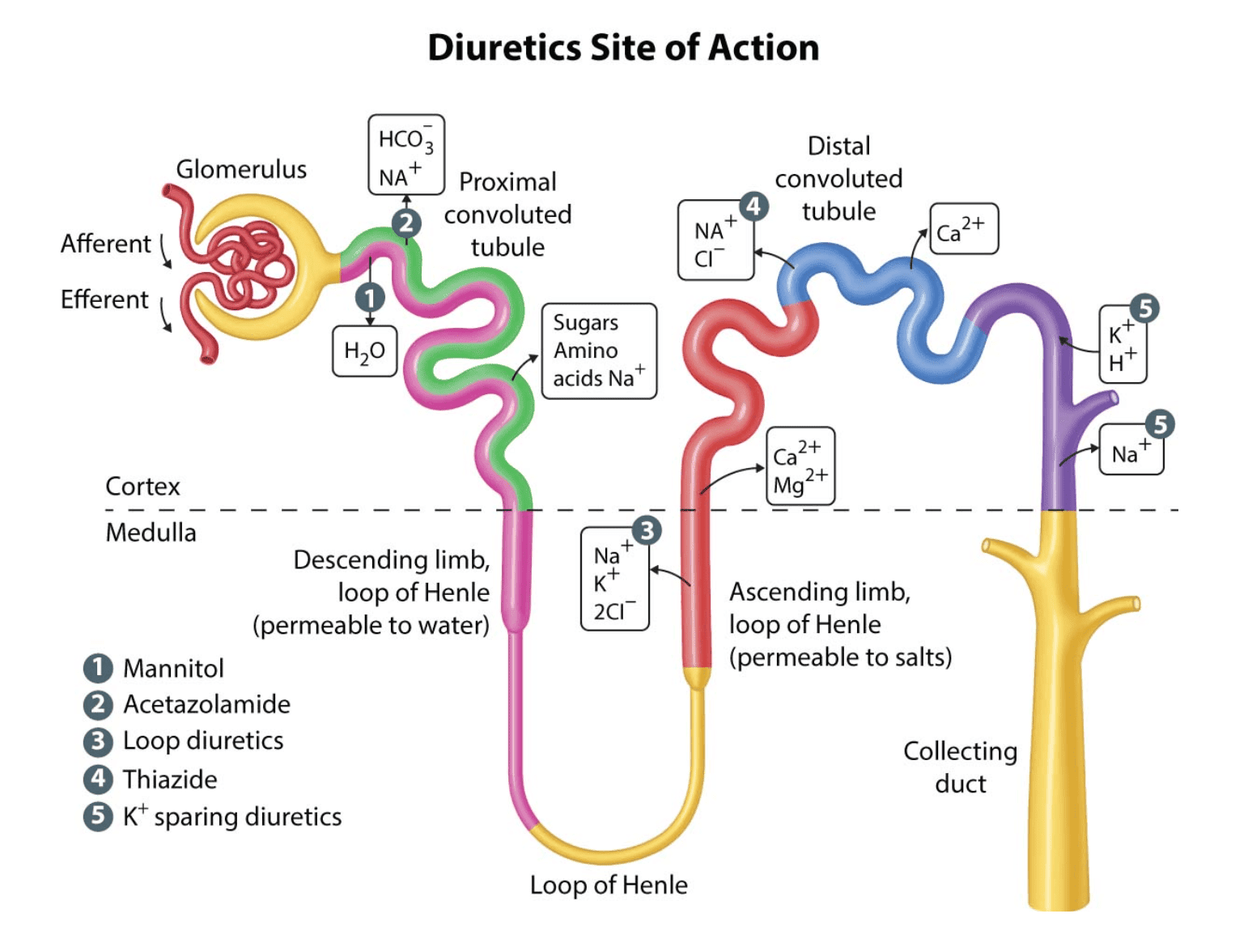
Thiazide diuretics such as hydrochlorothiazide are frequently used in the outpatient treatment of hypertension, especially in African American patients, as they have been shown to be especially beneficial in this population. Thiazides work by inhibiting sodium chloride reabsorption in the early part of the distal convoluted tubule (DCT) that serves to diminish the diluting capacity of the nephron and induces diuresis.
Thiazide diuretics have many adverse events, many of which involve electrolyte imbalances and metabolic disturbances. By inhibiting sodium reabsorption in the DCT, use of thiazide diuretics can result in hyponatremia, as was seen in this patient. In addition, calcium is reabsorbed within the DCT, and thiazide diuretics are known to enhance calcium reabsorption at these transporters. As such, thiazide diuretics will cause a decrease in calcium excretion and can cause hypercalcemia (as was also seen with this patient’s laboratory studies). For this reason, thiazide diuretics can also be used to treat patients with recurrent nephrolithiasis due to calcium-containing stones. However, they should not be used in patients with preexisting hypercalcemia.
Additional adverse events of thiazide diuretics include:
- Hyperglycemia
- Hypokalemia
- Hyperuricemia
- Metabolic alkalosis
- Hyperlipidemia
- Orthostasis
As such, it is important to schedule a patient for follow-up laboratory studies after initiating treatment with a thiazide diuretic. Also note that, in both clinical practice and on the USMLE, patients may have none, one, or multiple of these aforementioned adverse events.
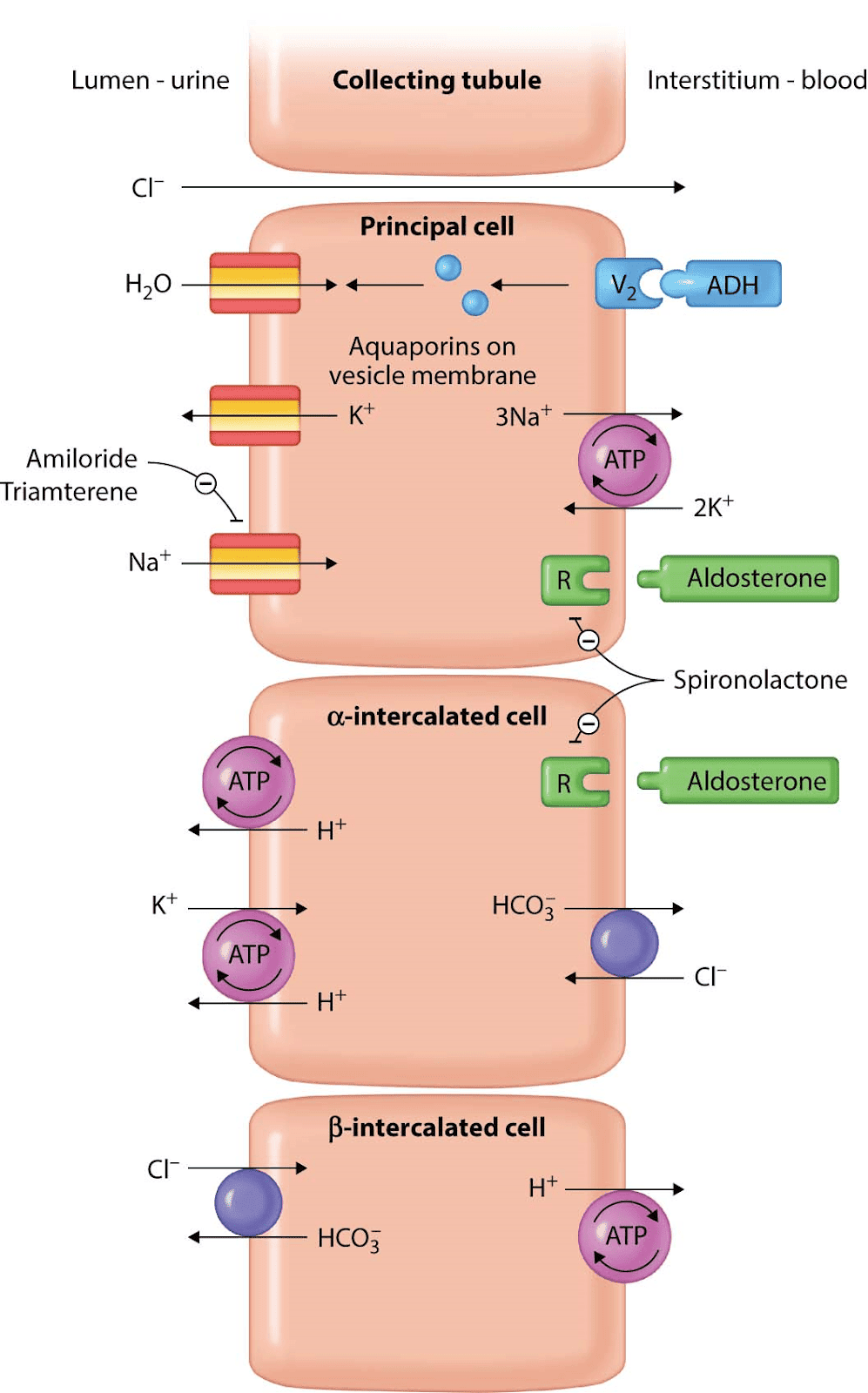
Answer A: Dihydropyridine calcium channel blockers, such as amlodipine, are often used in the treatment of hypertension as they cause vascular smooth muscle relaxation via blockage of voltage-dependent L-type calcium channels. Although they are calcium channel blockers, they are not associated with the development of hypercalcemia or hypocalcemia. Adverse events of these drugs include peripheral edema, weight gain, flushing, dizziness, and gingival hyperplasia.
Answer B: Angiotensin-converting enzyme (ACE) inhibitors, such as lisinopril, are frequently used in the outpatient treatment of hypertension. They are often used in patients with diabetes as these drugs are also nephroprotective in this population. Adverse events of ACE inhibitors include a dry cough, angioedema, and hyperkalemia. They are not associated with hypercalcemia.
Answer C: Beta-blockers are often used in the treatment of hypertension as they decrease both cardiac output and renin secretion. Beta-blockers decrease renin secretion via beta-1 receptor blockade of the juxtaglomerular apparatus cells. Beta-blockers do not cause hypercalcemia. Adverse events of beta-blockers include bradycardia, heart block, sedation, fatigue, exercise intolerance, erectile dysfunction, dyslipidemia (metoprolol only), and asthma or chronic obstructive pulmonary disease exacerbations (nonselective beta-blockers only).
Answer D: Hydralazine is an arterial dilator that may be used in the outpatient treatment of hypertension. Hydralazine causes vasodilation via increased cGMP, which results in smooth muscle relaxation. Given that its main effect is arterial dilation, use of hydralazine can result in rebound tachycardia. Additional adverse events include drug-induced lupus, fluid retention, headache, and angina. Hydralazine does not cause hypercalcemia.
Bottom Line: Thiazide diuretics are frequently used in the outpatient treatment of hypertension and work by inhibiting sodium chloride reabsorption in the distal convoluted tubule in order to induce diuresis. Thiazides also decrease calcium excretion and, as such, can result in the development of hypercalcemia.
For more information, see:
- Mechanism of action of diuretics: UpToDate
- First Aid for the USMLE Step 1 2019: 593, 595.
- First Aid for the USMLE Step 1 2020: 609.
TrueLearn Insight
Tip #1: If you struggle with multistep questions such as this, you can try working backwards from the answer choices. Here, you could have converted each answer to the medication whose mechanism of action it was describing. From there, you would ask yourself: (1) Would this be used to treat hypertension, and (2) could it cause hypercalcemia? Make sure to take advantage of this being a multiple-choice test and learn to work backwards on 2-step and 3-step questions.
Tip #2: The USMLE will frequently ask you questions about a medication without telling you what that medication is. Instead, you will need to identify it based on things like: what is it being used for or what laboratory changes and adverse events developed after using it. Make sure to know the medications that you would use for the treatment of common conditions such as hypertension, diabetes, and dyslipidemia.
Third Sample Question: Primary Sclerosing Cholangitis Risk Factors
A 40-year-old man presents for magnetic resonance cholangiopancreatography (MRCP) as part of ongoing evaluation for fatigue. He notes several other additional symptoms but is unsure if these are related, given that they have been present for many years. Laboratory studies had been ordered by his primary care physician and were remarkable for elevated alkaline phosphatase and direct bilirubin. He occasionally drinks a glass of wine or beer with dinner but denies tobacco or intravenous drug use. MRCP is performed and reveals a series of strictures and dilations in the intrahepatic and extrahepatic biliary ducts. This patient most likely has a history of which of the following additional symptoms?
- Abdominal pain and bloody diarrhea
- Dysarthria and tremor
- Epigastric pain that improves with meals
- Joint pain and hyperpigmentation
- Watery diarrhea
Explanation
The correct answer is: A
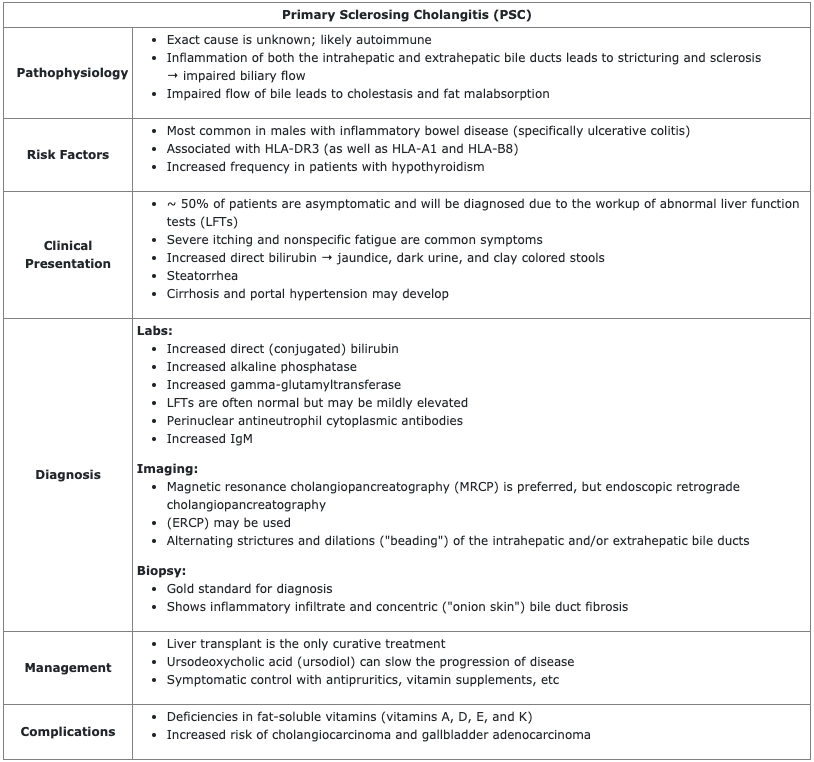
The MRCP findings seen in this patient are indicative of PSC, a form of biliary tract disease that results in concentric bile duct fibrosis of both the intrahepatic and extrahepatic bile ducts. Biliary fibrosis impairs the flow of bile, resulting in an increase in direct (conjugated) bilirubin and alkaline phosphatase on labs. Given that most patients are asymptomatic, PSC is often discovered incidentally due to the evaluation of these abnormal LFTs. When present, common symptoms include fatigue, jaundice, right upper quadrant pain, and steatorrhea.
MRCP or ERCP are useful for making a diagnosis and will demonstrate alternating strictures and dilations (“beading”) of the intrahepatic and/or extrahepatic bile ducts. A biopsy is useful for determining a definitive diagnosis and will show an inflammatory infiltrate as well as concentric bile duct fibrosis.
PSC is most common in male patients with a history of inflammatory bowel disease (most commonly ulcerative colitis); as such, this patient could have noted a prior history of abdominal pain and bloody diarrhea.
Answer B: Wilson disease is caused by an autosomal recessive mutation in the hepatocyte copper-transporting ATPase and results in decreased copper excretion into bile. Subsequent copper accumulation can affect the liver, brain, cornea, and kidneys. In the brain, copper frequently deposits in the basal ganglia and causes symptoms such as dysarthria, dystonia, tremor, and parkinsonism. Wilson disease is not a risk factor for PSC.
Answer C: The presence of epigastric pain that improves with meals is suggestive of a duodenal ulcer. Duodenal ulcers are commonly caused by Helicobacter pylori but may also be found in patients with a gastrinoma (Zollinger-Ellison syndrome). PSC does not increase the risk of duodenal ulcers.
Answer D: Hereditary hemochromatosis is caused by an autosomal recessive mutation that results in increased absorption of iron by enterocytes and symptoms secondary to iron deposition. Patients are frequently approximately 50 years of age and may complain of joint pain, new-onset type 2 diabetes mellitus, hyperpigmentation (“bronze diabetes”), loss of libido, hepatomegaly, jaundice, and cardiomyopathy. Hereditary hemochromatosis is not a risk factor for PSC.
Answer E: In patients with PSC, biliary fibrosis impairs bile flow and can result in fat malabsorption and the presence of steatorrhea. As a result of impaired fat absorption, patients are at risk of developing deficiencies in the fat-soluble vitamins (vitamins A, D, E, and K) and may present with associated symptoms. Watery diarrhea is not seen in patients with PSC.
Bottom Line: Primary sclerosing cholangitis (PSC) most commonly occurs in males with a history of ulcerative colitis. Diagnostic features of PSC include increased alkaline phosphatase and direct (conjugated) bilirubin on labs and imaging that shows dilation and strictures within the intrahepatic and/or extrahepatic bile ducts.
For more information, see:
- Primary sclerosing cholangitis in adults: Clinical manifestations and diagnosis: UpToDate
- First Aid for the USMLE Step 1 2019: 389.
- First Aid for the USMLE Step 1 2020: 395.
TrueLearn Insight
Make sure to understand the key differences between primary biliary cirrhosis and primary sclerosing cholangitis. Students frequently struggle to differentiate between these two pathologies on the USMLE exams.